Article Text

Statistics from Altmetric.com
Description
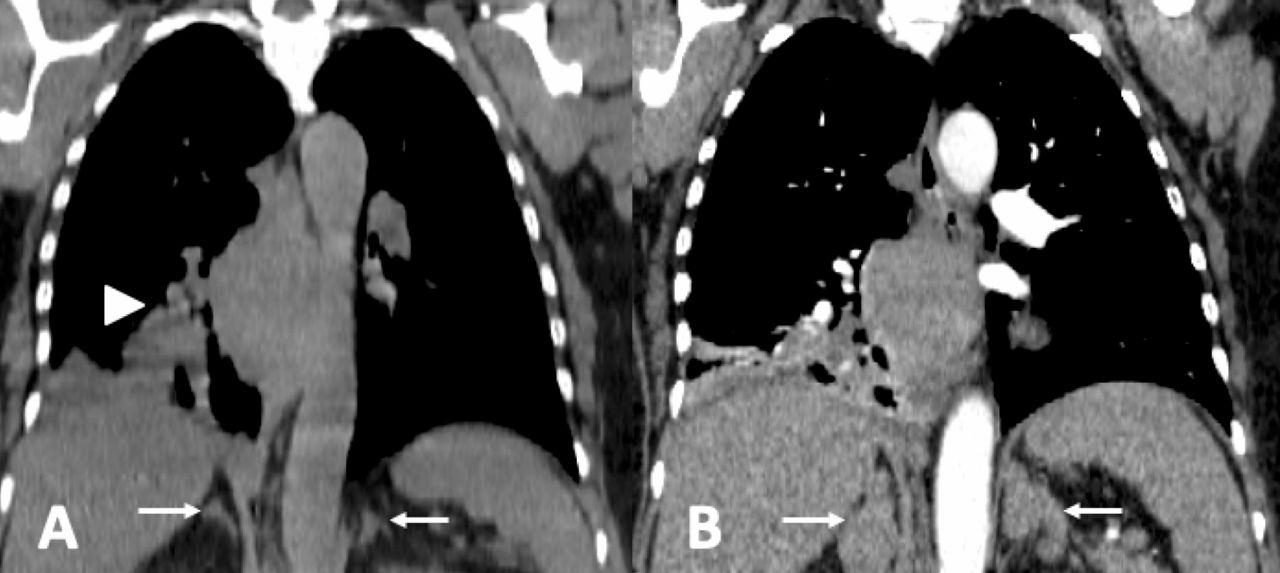
A 63-year-old woman with a smoking history of 20 pack-years presented with 3 months of weight loss. A right lung mass and uniformly enlarged adrenal glands were noted on computed tomography (figure 1A). A week later she developed severe hypokalemia (K 2.3 mEq/L, 3.5–5.5), hypertension and hyperglycemia. Endocrine testing demonstrated adrenocorticotropic hormone (ACTH) dependent hypercortisolemia: serum cortisol did not suppress with high-dose dexamethasone (65.4 µg/dL, <1.8), ACTH level was 56.6 pmol/L (2.2–13.3). Lung biopsy revealed small cell lung cancer (SCLC) and paraneoplastic Cushing’s syndrome was diagnosed. She needed aggressive potassium replacement and was treated with chemotherapy plus adrenal enzyme inhibition with metyrapone and fluconazole. Despite this, her condition progressed. The adrenal glands quadrupled in size over 8 weeks, measuring 6 cm in the largest dimension (figure 1B). Paraneoplastic ACTH can cause extreme cortisol elevations and massive adrenal enlargement, and has a poor prognosis.1 The median survival for patients with SCLC is 6.6 months with ACTH secretion compared with 13.1 months without ACTH secretion.1 The patient died 4 months after diagnosis.
{kind=link}
CT imaging demonstrated (A) bilateral enlarged adrenal glands (arrows) and right lung mass (arrow head) at initial presentation and (B) fourfold enlargement of the adrenal glands after 2 months.
Learning points
Small cell lung carcinoma (SCLC) is an aggressive neuroendocrine tumour with the capacity to secrete hormones, including adrenocorticotropic hormone (ACTH), resulting in Cushing’s syndrome.
SCLC with ACTH secretion carries a poorer prognosis than SCLC without paraneoplastic phenomena.
Extreme ACTH secretion causes massive adrenal stimulation leading to adrenal gland hypertrophy and excessive cortisol secretion, resulting in hyperglycemia, hypertension and hypokalemia.
Footnotes
Twitter @JenniferSnaith
Contributors Both JRS and CMG wrote and edited the manuscript. BG and DC edited the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.