Article Text

Statistics from Altmetric.com
Description
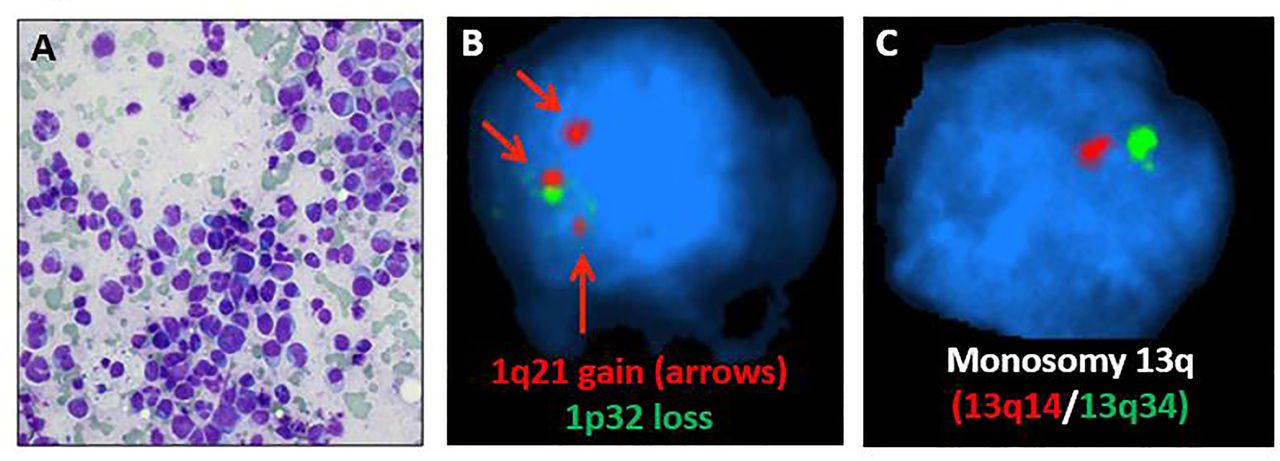
A 53-year-old HIV-negative man presented to the emergency room with a month of testicular pain, rapidly enlarging testes, night sweats and unintentional weight loss. He did not report any recent travel or sick contacts. Physical examination was remarkable for bilaterally enlarged testes to 8 cm and T7 dermatomal sensory loss. Pertinent laboratory studies revealed: haemoglobin 113 g/L (reference range, 135–180), IgG-lambda M-spike 3.4 g/dL and lactate dehydrogenase (LDH) 705 IU/L (reference range, 140–280). Positron emission tomography/computed tomography (PET/CT) (figure 1) showed hypermetabolic testicular masses, extensive lytic bone lesions, epidural metastases at T7, T8, T12 and L3 with cord impingement at T7−T8, and a large left iliac mass, and bilateral perinephric masses. Biopsy of a perinephric mass showed atypical cells with lambda light-chain restricted plasma cells. A bone marrow biopsy (figure 2A) showed 40% anaplastic plasmacytoid cells with pleomorphic morphology consistent with plasmablastic myeloma. The large plasmablastic cells were CD38(+), CD138(+), MUM1(+), CD20(−), CD30(−), CD45(−), PAX-5(−), ALK-1(−), EBER-ISH(−) and HHV8(−), with a high Ki-67 staining 90% of the cells. Fluorescent in situ hybridization (FISH) was pertinent for chromsomes 13q deletion, 1 p deletion and trisomy 1q (figure 2B and C), which are commonly associated with multiple myeloma. The differential diagnosis included plasmablastic myeloma, plasmablastic lymphoma and anaplastic myeloma. Given the bone marrow morphology, extranodal findings, lack of Epstein Barr Virus (EBV) and Human Herpesvirus-8 (HHV8) involvement, as well as myeloma-associated FISH abnormalities, the diagnosis was more consistent with plasmablastic myeloma. Following a short course of external radiation to the T7−T8 spine, systemic treatment included a combination of the anti-CD38 monoclonal antibody daratumumab along with cyclophosphamide, doxorubicin, vincristine, and prednisone every 3 weeks, which resulted in partial response after three cycles, indicated by a reduction M-spike to 0.7 g/dL. In addition, his total IgG decreased from 5.6 to 1.1 g/dL, serum lambda light chain decreased from 460 to 76 mg/dL. Unfortunately, he later decompensated due to severe sepsis secondary to pneumonia, leading to respiratory failure and death.

Positron emission tomography/computed tomography (PET/CT) results. PET-avid areas showing diffuse skeletal and soft tissue uptake.
{kind=link}
{kind=link}
Pathologic findings. Morphology of plasmablastic cells on bone marrow aspiration (A) and cytogenetic abnormalities on fish showing gain of 1q21 and loss of 1p32 (B) as well as deletion 13q (C).
Plasmablastic myeloma is rare and morphologically similar to plasmablastic lymphoma, but is typically EBV-negative, and portends a poor prognosis with a reported median survival of 10 months.1 2 Given the low incidence of plasmablastic myeloma, there is no consensus on management of newly diagnosed patients. Treatment typically includes a combination of modern anti-myeloma agents, such as the proteasome inhibitor bortezomib, along with chemotherapy.3 In the Myeloma E9486 trial, the largest interventional study on plasmablastic myeloma, treatment with vincristine, carmustine, melphalan, cyclophosphamide and prednisone showed a response rate of 47%.1 To the best of our knowledge this is the first report of plasmablastic myeloma treated with a regimen that included daratumumab, which resulted in a partial response. An ongoing early phase 1 clinical trial (NCT04139304) is examining the benefit of daratumumab combined with etoposide, prednisone, vincristine, cyclophosphamide and doxorubicin.
Learning points
Plasmablastic myeloma is a rare and aggressive neoplasm presenting with overlapping features of multiple myeloma and non-Hodgkin's lymphoma.
There is no consensus on the management of plasmablastic myeloma.
When combined with chemotherapy, the anti-CD38 monoclonal antibody daratumumab may effectively target plasmablastic myeloma cells.
Footnotes
Twitter @docbraunstein
Contributors JAS-L and MJB both managed the patient and drafted the manuscript. AR and CA-P helped draft the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MJB reports research funding from Janssen and serves on advisory boards for Amgen, AstraZeneca,Celgene, Janssen, Karyopharm, Takeda and Verastem. JAS-L has served on advisory boards for Amgen, AstraZeneca, Celgene and Verastem.
Patient consent for publication Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.