Article Text

Statistics from Altmetric.com
Description
A 41-year-old healthy woman, gravida 2 para 2, was referred to our gynaecological outpatient department due to her history of menorrhagia, with 6 months of evolution, and with consequent anaemia (haemoglobin—95 g/L). During gynaecological examination, a 12-week uterus was palpable and a pelvic ultrasound showed an augmented uterus (104×74×60 mm) with multiple submucous myomas (the larger with 22 mm). The patient started taking ulipristal acetate to achieve uterine bleeding control while waiting for hysteroscopy. Three weeks after, she was admitted to the emergency department due to ongoing heavy uterine bleeding with a symptomatic anaemia (haemoglobin—88 g/L). Facing this medical resistant intense uterine bleeding and no fertility preservation desire, total hysterectomy was performed after transfusion of one unit of red blood cells.
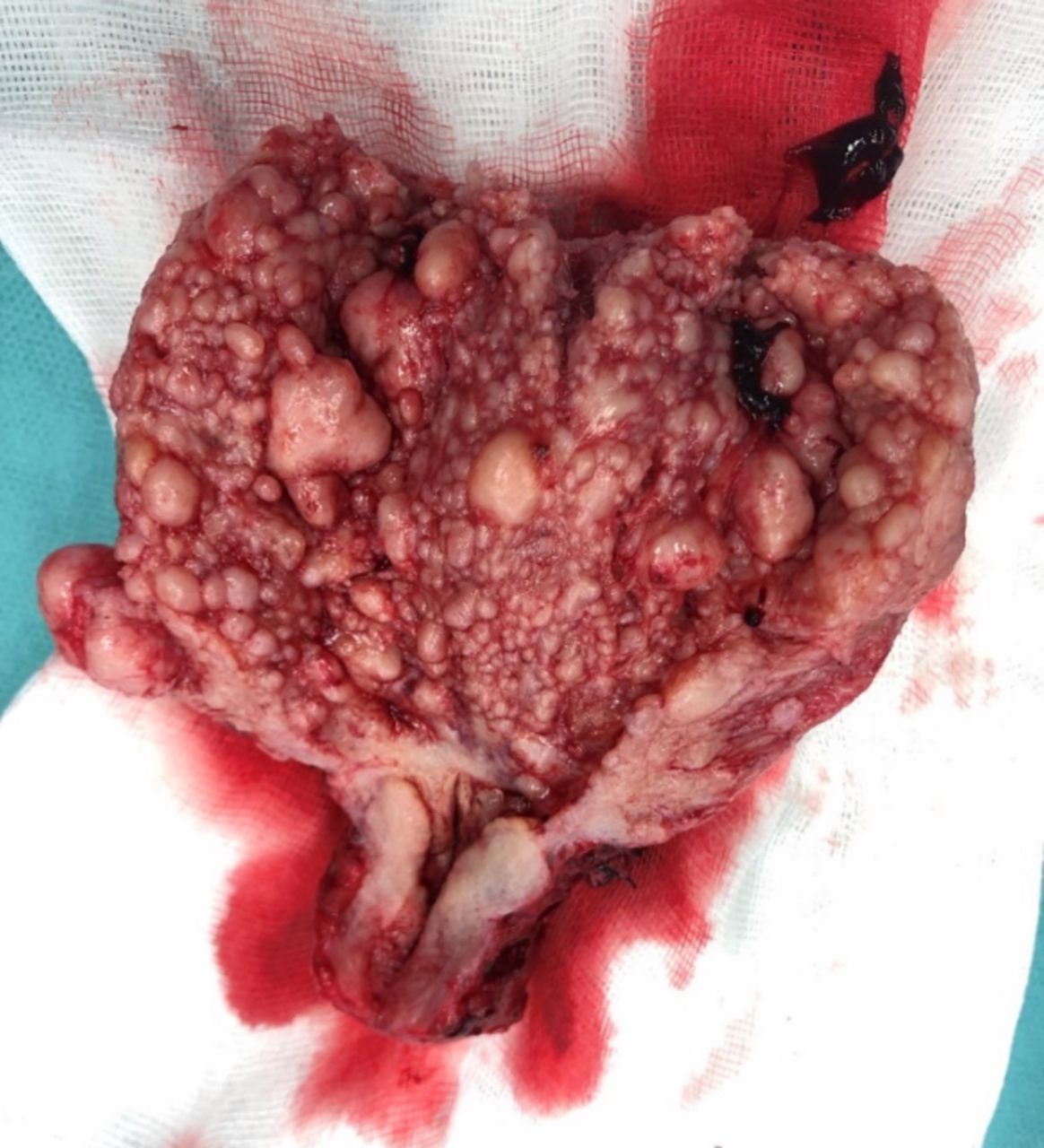
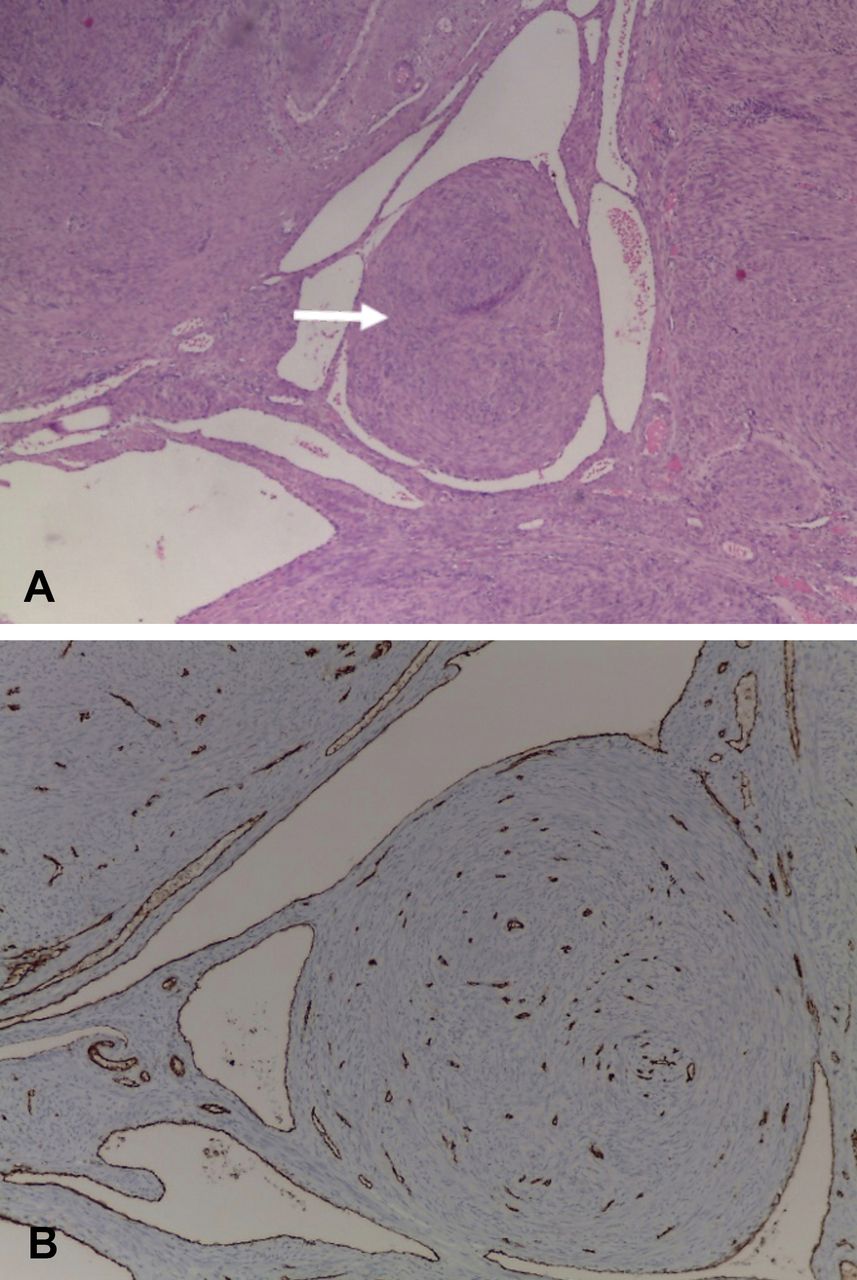
Surgical examination showed a slightly increased uterus, without visible myomas, and with macroscopically normal adnexa. Histological examination revealed multiple macroscopic intracavitary/intramural myomas ≤1 cm (figure 1); microscopy of these myomas displayed features compatible with intravenous leiomyomatosis (IVL) (figure 2A,B). Echocardiogram, high-resolution pulmonary CT and pelvic MRI were sequentially performed but showed no additional findings. The patient started taking continuous oral progestogen and remains asymptomatic 6 months after surgery.

Interior part of surgical specimen, showing a particular aspect of the endometrial cavity occupied by multiple nodular structures.

{kind=link}
{kind=link}
(A) Nodular smooth muscle tumour (H&E, ×4). (B) Endothelial vascular walls stained with CD31 marker, confirming the intravenous component of leiomyomatosis (×10).
IVL is a rare condition with about 300 cases reported before 2020 and since its first description in 1896 by Birch-Hirschfeld.1 Although histologically benign, this uterine neoplasm is characterised by venous smooth muscle nodular growing with potential extension to the inferior vena cava, right heart cavities and pulmonary arteries, where it can lead to embolic phenomena, heart blockade and death. Most reported cases describe diagnosis in the fifth decade of life with special incidence in the perimenopausal stage, although 20–80-year-old women have been diagnosed.2 3 Because in its early stages IVL can be asymptomatic, or its clinical features can overlap those of myomatous uterus (hypermenorrhoea, pelvic discomfort, pelvic mass), it can be underdiagnosed or diagnosed after cardiac/vascular involvement.2–5 Complete resection of all existing tumours is the adequate treatment for IVL, with total hysterectomy and bilateral salpingo-oophorectomy being recommended to treat pelvic disease.2 4 6 Bilateral oophorectomy is controversial if the disease is confined to the uterus in <40-year-old women.7 Early uterine histological diagnosis should prompt proper investigation to exclude extrapelvic involvement; echocardiography is the gold standard to identify intracardiac leiomyomatosis and thoraco-abdominal-pelvic CT or MRI is recommended to evaluate the extent of tumour involvement, with vascular reconstruction allowing determining the location, size and full extension pathway of IVL lesions.2 3 The recurrence rate may be as high as 30% and it depends on the age of the patient and initial size of the tumour.2 7 To reduce this risk, drug therapy with gonadotropin-releasing hormone agonists, tamoxifen or medroxyprogesterone is being controversially proposed, mainly in cases of incomplete resection. Long-term follow-up with CT or MRI is advised by most authors, and in the absence of periodicity recommendations, annual evaluations are currently proposed, with recurrences described up to 15 years after diagnosis and resection.2 6 7
Learning points
Intravenous leiomyomatosis is a rare condition, difficult to suspect before gynaecological surgery and when there is no extrapelvic involvement.
When diagnosis is accidentally made following hysterectomy, clinical investigation should be performed for the early diagnosis of potentially fatal cardiac and vascular involvement.
Gynaecological long-term follow-up must be offered to prevent fatal recurrence events.
Footnotes
Contributors RPM: surgical intervention, planning, conducting and reporting of the work; CU: patient follow-up and review of the work; AIB: histological diagnosis and review of the work; FG: surgical intervention and review of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.