Article Text

Statistics from Altmetric.com
Description
A 68-year-old woman with a 22-year history of idiopathic pulmonary hypertension presents for coronary angiography after a nuclear stress test revealed an apical defect. Evaluation was prompted by worsening dyspnea on exertion.
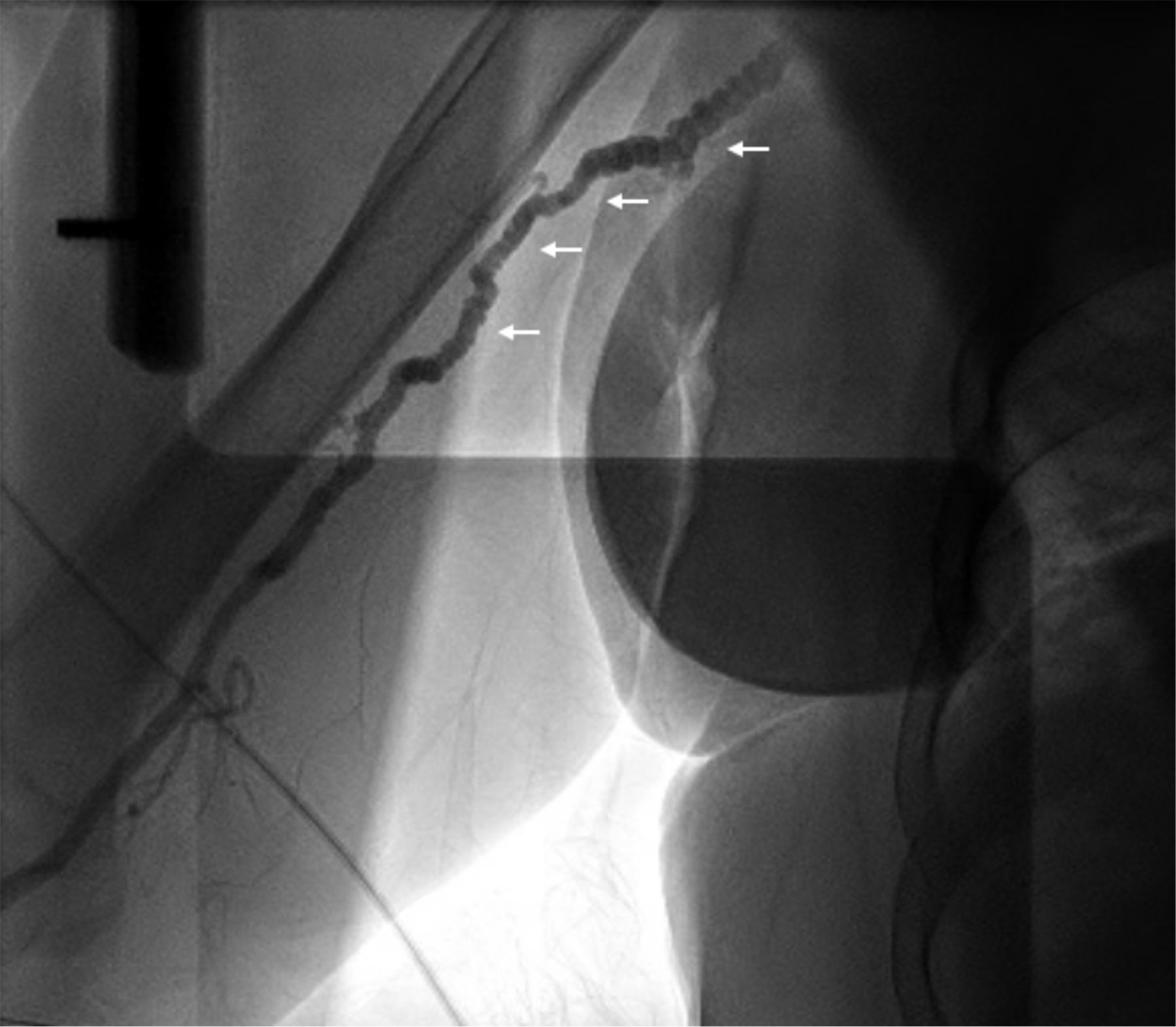
During angiography, fibromuscular dysplasia (FMD) was noted in the long segment of the right brachial artery (figure 1), resulting in difficulty navigating the catheter. She also had a left ventricular aneurysm in the mid-anterior wall and an arteriovenous fistula between the mid-left anterior descending artery and the pulmonary artery (figure 2). The right heart catheterisation revealed that she had severe pulmonary hypertension (PA pressure 60/32 mm Hg, mean pressure 43 mm Hg) without left to right shunt. The cardiac output and cardiac index were 3.17 L/min and 1.7 L/min/m2, respectively. Coronary arteries were patent and the left ventricular ejection fraction was normal.

Fibromuscular dysplasia of the right brachial artery, with classic ‘bead on a string’ appearance.
{kind=link}
{kind=link}
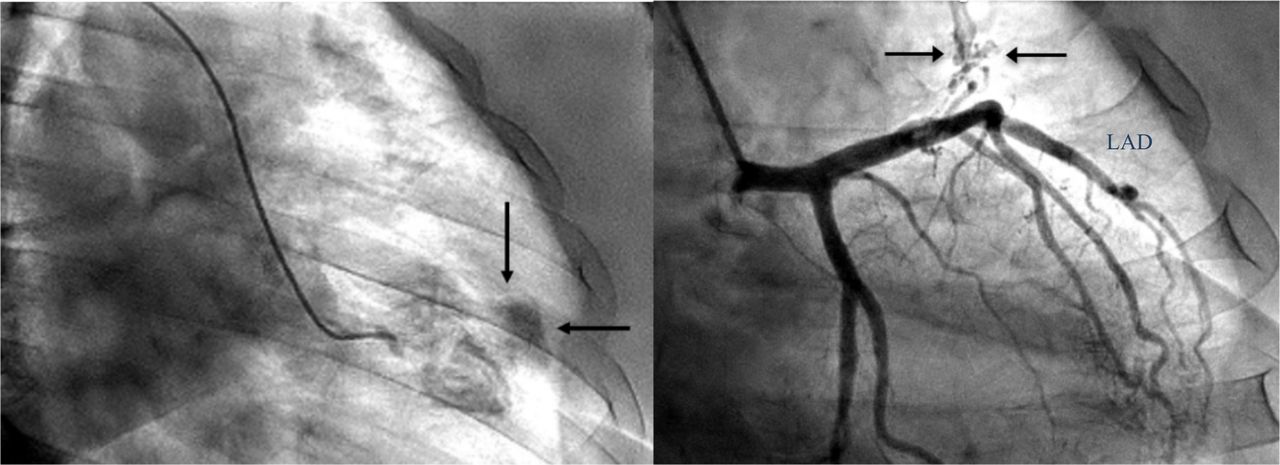
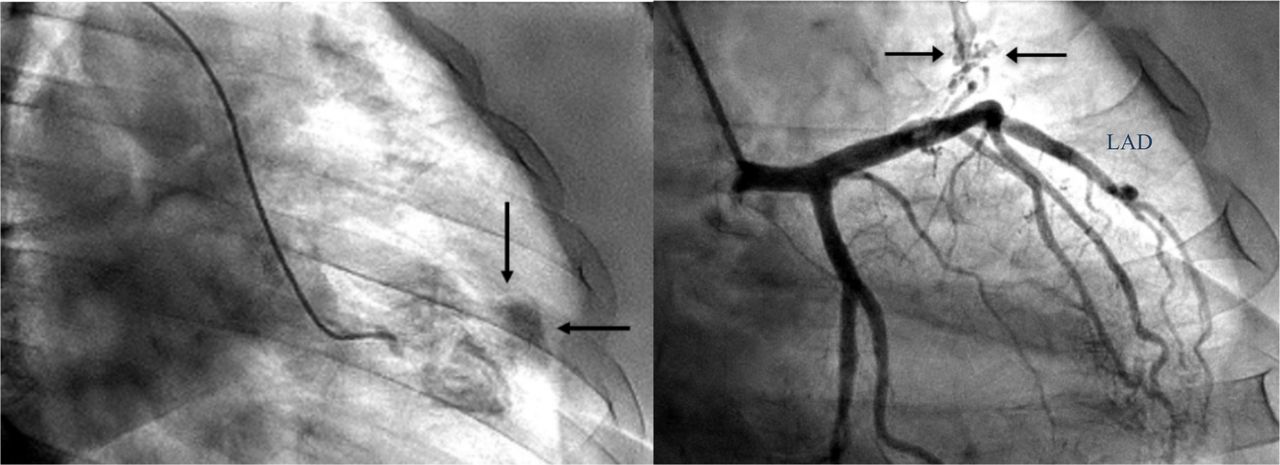
Left panel: left ventricular aneurysm, denoted by the arrows. Right panel: coronary angiography with black arrows denotes the fistula between the mid-left anterior descending artery (LAD) and the pulmonary artery, blue arrow denotes the LAD.
Serial imaging from the past decade revealed progressive aneurysmal dilatation of the pulmonary arteries. The main pulmonary artery measures 4.6 cm in transverse diameter; left and right branches are both 4.0 cm. In addition, she had bilateral common iliac artery aneurysms, 2.1 cm on the left and 1.8 cm on the right.
Ultimately, no invasive interventions were taken and the patient was optimised on medical therapy consistent of ambrisentan, tadalafil and sildenafil with symptomatic improvement. On follow-up, she was found well and reported a good quality of life.
Fibromuscular dysplasia
FMD is a non-atherosclerotic, non-inflammatory arteriopathy that typically affects middle-aged women. Although commonly reported in renal and cervicocephalic arteries, they can be found in virtually all arteries, though the upper extremities involvement is very rare.1 FMD can lead to stenosis, aneurysms, dissection, arteriovenous fistula formation and thrombotic events of both the affected vascular bed and distant vessels.1–4 While FMD increases the risk of systemic hypertension, its association with pulmonary hypertension is less clear. There have been reports of disseminated FMD leading to pulmonary hypertension via stenosis or thromboembolism in the pulmonary arteries.5 6 It is possible that our patient’s pulmonary hypertension originated via a similar mechanism but was not captured on imaging. We also hypothesise that FMD was a predisposing factor for the development of diffuse vasculopathy in this patient, possibly contributing to the progressive dilation of the pulmonary artery aneurysm.
Finally, according to recent recommendations,3 patients with FMD should undergo imaging to identify other affected vasculature and to screen for occult aneurysms and dissections. Low-dose aspirin may be reasonable for preventing thrombotic complications. Our patient was already on anticoagulation for atrial fibrillation, so aspirin was not added.
Coronary artery fistulas
Coronary artery fistulas (CAF) are rare and abnormal connections between a major vessel and other cardiac chambers. They are usually diagnosed incidentally on angiography.7 While most are asymptomatic, CAFs can result in angina, congestive heart failure and arrhythmias. For our patient, the fistula appeared to have no haemodynamic consequence at the time of angiography, thus a conservative approach was taken. However, the abnormal connection between a coronary artery and the pulmonary artery has the potential to worsen her pulmonary hypertension. If the CAF becomes haemodynamically significant, blood would flow from the coronary vessel to the lower pressure circulation, increasing the pulmonary artery pressure. Therefore, if the patient develops cardiac or respiratory symptoms in the future, she may warrant workup to evaluate for haemodynamic significance of the CAF. If necessary, many treatment options are available, ranging from transcatheter embolisation to surgical closure.8
Patient’s perspective
I have been diagnosed with idiopathic pulmonary hypertension for over 20 years and was originally only given 3–5 years to live. Even though there are still no clear explanation for my disease, the findings here may bring us one step closer. I am grateful that the authors took the time to explain the imaging results in detail. These vascular findings may become important in my care in the future.
Learning points
Patients with fibromuscular dysplasia (FMD) are at increased risk for vascular sequelae at distant vessels and should undergo screening for occult aneurysms, arteriovenous fistulas and dissections.
Use of prophylactic aspirin should be considered for patients with FMD to prevent thrombotic complications.
Coronary artery fistulas are often asymptomatic but can lead to cardiac sequlae. The onset of symptoms warrant evaluation for haemodynamic significance of the fistula and may merit repair.
Footnotes
Contributors ME-H provided care for the patient. WQZ and SK planned and drafted the manuscript. ME-H critically reviewed the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.