Article Text

Statistics from Altmetric.com
Description
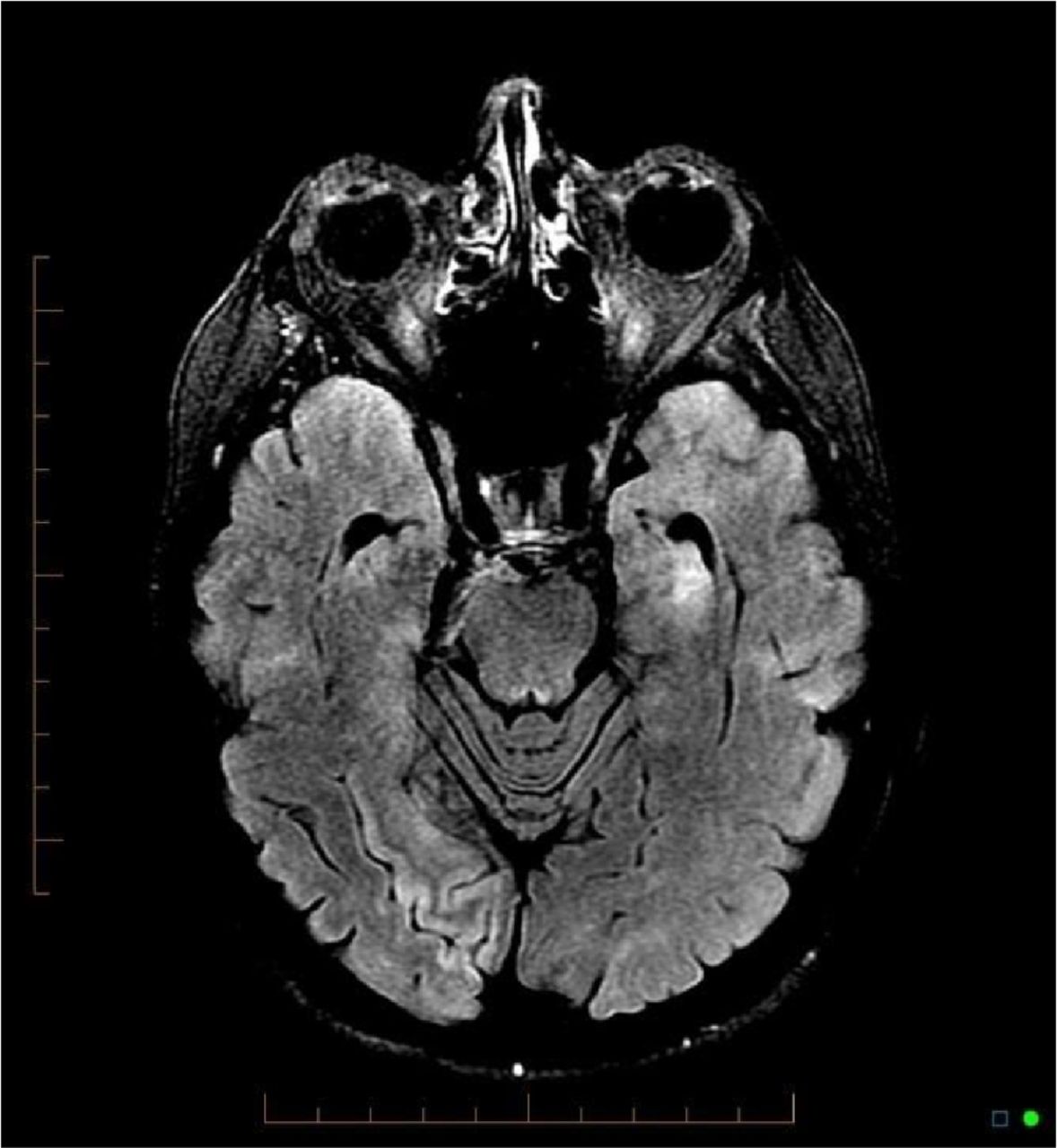
A 76-year-old, right-handed, Caucasian woman presented with influenza A and diarrhoea. Medical history includes trigeminal neuralgia, dyslipidaemia, hypertension and hypothyroidism. The patient’s regular medications included thyroxine, atenolol, atorvastatin, pregabalin and valproate. Family history was unremarkable. A CT abdomen pelvis was performed to investigate diarrhoea. Incidentally, the patient was found to have multiple renal infarcts (figure 1). This was in the setting of new-onset atrial fibrillation, presumably due to infection. Bloods revealed elevated lactate dehydrogenase (LDH) consistent with acute renal infarcts and preserved renal function. Subsequently, she was found to have confusion, poor calculation, recall and a left upper homonymous quadrantanopia. She proceeded to have an MRI brain. This revealed multiple vascular territory infarcts, which involved in the right mesial temporal lobe extending to the occipital lobe, left thalamus and left mesial temporal lobe (figure 2). Specific neurology matched the territories infarcted, demonstrated well on figure 2. This woman was anticoagulated for her atrial fibrillation with apixaban. Unfortunately, her cognitive impairment has persisted.

Multiple renal infarcts.
{kind=link}
{kind=link}
MRI fluid attenuation inversion recovery (FLAIR)—multiple cerebral infarcts.
Patient’s perspective
Given patient’s persistent cognitive impairment, we gained some perspective from the patient and her husband (and carer):
Patient: Thank goodness it wasn’t worse than it was, in that I don’t need a walking stick or anything like that.
Patient’s husband: It has affected memory, increased anxiety, and has certainly affected her cognitive ability but has not affected her physical ability, and in that respect I feel this is a slight stroke and she got off lightly. The effect on vision is not severe. I’m lucky, it could have been so much worse. Surprised by the diagnosis as had put it down to symptoms of flu and a recent cruise.
Learning points
The renal infarcts were silent in that there was no pain, no rise in serum creatinine, and the lactate dehydrogenase (LDH) rise could be considered non-specific. Her confusion could have been attributed to delirium in the context of acute infection and her cerebral infarcts may have easily gone undetected.
The areas of infarct involved multiple vascular territories, supporting an embolic aetiology, likely secondary to atrial fibrillation. However, for completeness thrombophilia, vasculitic and antiphospholipid screens were done and found to be negative.
How often is this occurring? And how often do they occur together? This case reports highlights the need to have a low threshold for neuroimaging in patients with new-onset neurological deficits, including delirium, in the setting of other systemic areas of infarction and in the presence of other risk factors for embolism including atrial fibrillation. The case also highlights the clinical utility of assessing LDH. It is the first to our knowledge of silent renal infarction presenting in association with cerebral infarction, with preserved renal function, although we suspect that this is both an under-recognised and underappreciated clinical phenomenon. Previous cases have been reported but patients were symptomatic or developed renal impairment associated with the renal infarcts.1–3
Footnotes
AP, RB and DS contributed equally.
Contributors The initial manuscript was drafted by AP, with editing by both DS and RB. GA (consultant radiologist) gave advice regarding image selection. Information was gathered by first three authors listed and RB obtained consent from the patient.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.