Article Text

Statistics from Altmetric.com
Description
A 61-year-old patient with diabetes mellitus, alcohol abuse and no prior admissions presented with an acute febrile illness (40°C) associated with rigours, nausea and epigastric pain. He had neither obesity nor hypertension, and was being treated by diet only, despite associated dyslipidaemia. On examination, sinus tachycardia (117/min) and tachypnoea (with oxygen saturation 99%) were noted, but the abdomen showed only diffuse tenderness without rebound, distention or hepatomegaly. Chest X-rays were normal.
Haemoglobin was 139 g/L (later, 108 g/L), WBC 4.8×109/L (later, 14.1×109/L), platelets 106×109/L (later, 570×109/L), C-reactive protein (CRP) 332 mg/dL, BUN 41 mg/dL, creatinine 1.6 mg/dL (later, 0.9 mg/dL), albumin 2.8 g/L, globulins 2.6 g/L (later, 3.7 g/L globulins), mildly increased transaminase levels, direct bilirubin 0.94 mg/dL, normal amylase and coagulation. Abdominal ultrasound demonstrated a large (12.5×8.0×11.8 cm) lesion in an otherwise normal liver. Given the predominantly solid appearance of the lesion and the nonspecific sonographic features (figure 1A), further imaging was recommended to differentiate between hepatic tumour and an abscess. Even after triple-phase CT differential diagnosis included hepatic tumours (eg, biliary cystadenoma, cystadenocarcinoma and intrahepatic cholangiocarcinoma) and liver abscess of either pyogenic or parasitic aetiology (figure 1B). MRI confirmed the diagnosis of an abscess (figure 1C–H). CT-guided percutaneous aspiration yielded 120 mL of thick purulent fluid positive for Klebsiella pneumoniae alone on BioFire panel and culture. Blood cultures later grew K. pneumoniae sensitive to many antibiotics.
{kind=link}
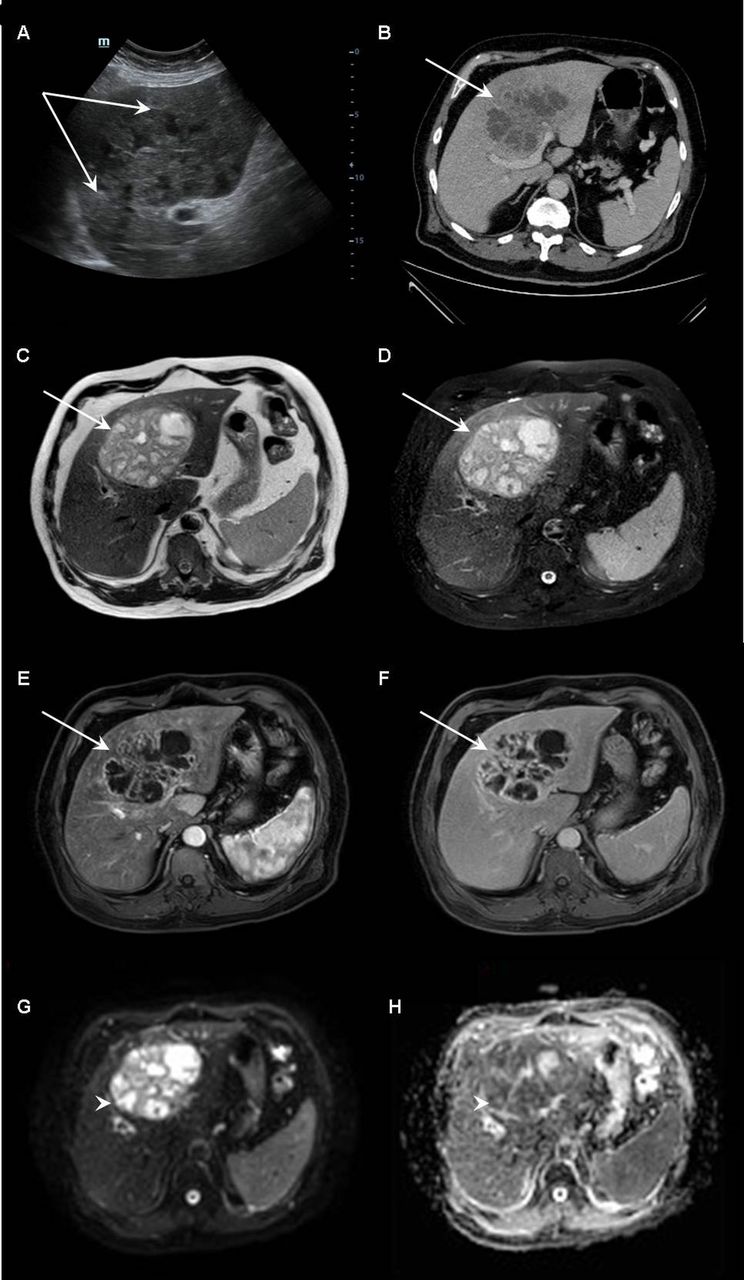
Complex solid and cystic hepatic lesion—US image (A) of the liver showed a large heterogeneous mass lesion, isoechoic to the liver with small hypoechoic spaces (arrows). Contrast enhanced CT image (B) showed multiloculated mass with thick enhancing internal septa (arrow). To better characterise the lesion prior to invasive intervention, MRI was performed. MRIs (C–G) show a complex mass with variable intensities of the inner collections on the T2-weighted images (arrows on C and D) and progressive enhancement (arrows on E and F). Diffusion-weighted imaging (DWI) (G) and apparent diffusion coefficient image (ADC map) (H) shows high signal intensity on diffusion-weighted images and hypointensity on ADC map of most of the internal cystic spaces supporting the leading diagnosis of a pyogenic liver abscess. Percutaneous drainage was performed with a final diagnosis of Klebsiella pneumoniae liver abscess (A—Grey scale US image, B—CT image with contrast on portovenous phase, C—T2-weighted image, D—spectral attenuated inversion recovery, E—T1-weighted image with fat suppression and contrast on arterial phase, F—T1-weighted image with fat suppression and contrast on late phase, G—apparent diffusion coefficient map and H—diffusion-weighted image).
Drainage catheter was left in place for 18 days and 4 weeks parenteral ceftriaxone/metronidazole were followed by 2 weeks oral amoxicillin/clavulanic acid. HIV and Entamoeba histolytica tested negative. Transesophageal echocardiography and colonoscopy were normal. He recovered (CRP 12 mg/dL) but had a recurrent small abscess 1 month later that responded to the same treatment with subsequent uneventful follow-up.
Pyogenic liver abscess (PLA), the most common visceral abscess, usually develops by portal vein pyaemia from an abdominal focus (or peritonitis) or a direct spread of biliary tract disease,1 and less often through the systemic circulation by haematogenous seeding of a systemic infection. The incidence of PLA was reported as 3.59/100 000 population/year in the USA,2 and this rate is increasing, with mostly mixed enteric facultative and anaerobic species and more iatrogenic interventions implicated being important recent trends.2
In our patient, the abscess had several peculiar characteristics: first, a single microorganism was involved (K. pneumoniae) whereas most PLA are polymicrobial.2 Second, the pathogenesis remained obscure: there was no evidence of infective endocarditis, no prior abdominal disease and no biliary tract disease, pancreatic pathology, colorectal neoplasia, diverticulitis or other abdominal focus of infection which are found in most of the patients with PLA. Lastly, its size 12.5 cm was consistent with a ‘giant abscess’ versus a mean of 7 cm.1
Our patient’s diabetes and alcohol abuse are recognised risk factors for PLA,1–3 but nevertheless, the abscess here remains cryptogenic and unusual. In this context, noninvasive vs invasive K. pneumoniae liver abscess syndrome must be considered. The latter, recently-described distinct clinical entity is characterised by its geographical distribution (mostly Asian patients, especially from Taiwan) and high frequency of seeding causing metastatic infections such as meningitis, endophthalmitis or lung abscess.4 Most patients are immunocompetent, do not have a predisposing gastrointestinal disease and the infection is monomicrobial with a high prevalence of virulent K. pneumoniae serotypes K1 or K2.5 In contrast, our patient’s presentation is consistent with the rare cryptogenic noninvasive K. pneumoniae-associated liver abscess syndrome: these cases involved isolated monomicrobial liver abscesses without the extrahepatic complications.4 The ‘giant’ monomicrobial liver abscess described here, was also discovered in the USA, although mostly in patients from Southeast Asia,4 and remains cryptogenic, a not uncommon diagnosis reported in a significant minority of patients in some series.2
CT remains best for diagnosis of PLA as the patient’s presentation may be nonspecific. Unique cases as in our patient may require MRI confirmation since the differential diagnosis of a liver mass with cystic components and internal septa includes liver malignancy and parasitic diseases where an aspiration may be harmful.6 Most ‘idiopathic’ cases can be effectively managed without surgery nowadays, by a combination of ongoing drainage and prolonged, organism(s)-tailored antibiotic treatment, and show a good prognosis.
Patient’s perspective
I was referred with high fever. That happened to me before. When they let me see the scans I could hardly believe I had this giant ball in my liver… It took time, but I am well now. I only hope it does not come back
Learning points
Before designating pyogenic liver abscess as cryptogenic, a thorough search must be made for an occult colorectal neoplasia, pancreatico-biliary disease (infectious or malignant) or other abdominal focus of infection seeding the liver.
A monomicrobial pyogenic liver abscess with Klebsiella pneumoniae mandates consideration of the recently described cryptogenic invasive K. pneumonia liver abscess syndrome, especially in Asians and when metastatic infections are associated, or its rare noninvasive variant.
Management based on prolonged organism-directed antibiotic treatment and ongoing radiological aspiration and drainage is usually curative.
Footnotes
Contributors AS wrote the manuscript. ID, TF and LU participated in its preparation. LU interpreted and prepared the images.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.