Article Text

Abstract
A 38-year-old man presented with a 2-month history of pain and stiffness in the bilateral wrist. The pain in right wrist was disabling and severe enough to restrict the daily life activities. After the evaluation of clinical and radiological features, the patient was diagnosed with Kienböck’s disease Lichtman stage IIIB in the right wrist and stage IIIA in the left wrist. Routine laboratory investigations revealed a serum uric acid 9.27 mg/dL. Lunate excision and scaphocapitate fusion were done in the right wrist after discussing with the patient. The histopathological examinations of tophi in synovial tissue were negatively birefringent under polarised light microscopy. It confirmed the diagnoses of gout. Febuxostat was started postoperatively. The patient returned to work at the end of 5 months. There was no recurrence of symptoms and radiological signs of arthritis at the end of 1 year.
- orthopaedic and trauma surgery
- rheumatology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Osteonecrosis is a disorder that usually affects adults aged 20–40 years. The hip, knee or shoulder is the familiar site of involvement. Avascular necrosis of lunate bone (Kienböck’s disease) is a relatively rare disease and influenced by multiple factors. The exact cause of avascular necrosis of lunate bone is not known. Several local and systemic risk factors have been defined for this disease. Negative ulnar variance is a well-recognised local factor found to be implicated in the pathogenesis of Kienböck’s disease.1 The association of Kienböck’s disease also described with several inflammatory disorders, such as systemic lupus erythematosus,2 sickle cell anaemia,3 scleroderma,4 rheumatoid arthritis,5 dermatomyositis6 and gout.7–9
Kienböck’s disease is usually seen in a unilateral dominant wrist. The incidence of bilateral Kienböck’s disease reported in the previous series is very low (3%–7%).10 No risk factor has been defined for bilateral disease. Osteonecrosis of the femoral head in gout with predominantly bilateral involvement is well reported.11 Osteonecrosis of lunate bone is relatively rare in gout, and only three cases of Kienböck’s disease in combination with gouty arthritis have been described in the literature.7–9 All these described cases are unilateral. To the best of our knowledge, this is the first report of bilateral Kienböck’s disease concomitant with gouty arthritis.
Case presentation
A 38-year-old man presented with complaints of pain and stiffness in the bilateral wrist for 2 months. The symptoms were more pronounced in the right wrist than the left wrist. The pain was insidious in onset, dull boring, which gradually increased in the last 2 months. The location of the pain was over the dorsum of both the wrists and the intensity of pain increased with the wrist movements. There was no diurnal variation in pain intensity. The patient used to take tablet paracetamol (1 g) whenever he felt an increase in pain intensity. There was no medical history of corticosteroids intake, occupation causing repetitive microtrauma, collagen disorder or prior history of pain in the first metatarsophalangeal (MTP) joint. There was minimal swelling and tenderness over the dorsal aspect of the right wrist. There was mild tenderness over the dorsum of the left wrist, and the range of motion of the left wrist was normal. The range of motion of the right wrist was painful and restricted. The active motion was as extension: 0°–30°, flexion: 0°–20°, ulnar deviation: 0°–10° and radial deviation: 0°–10°. The preoperative Mayo wrist score was 35 points, and the pain was 1.5 according to the visual analogue scale. The grip strength was 23% in the right hand.
Investigations
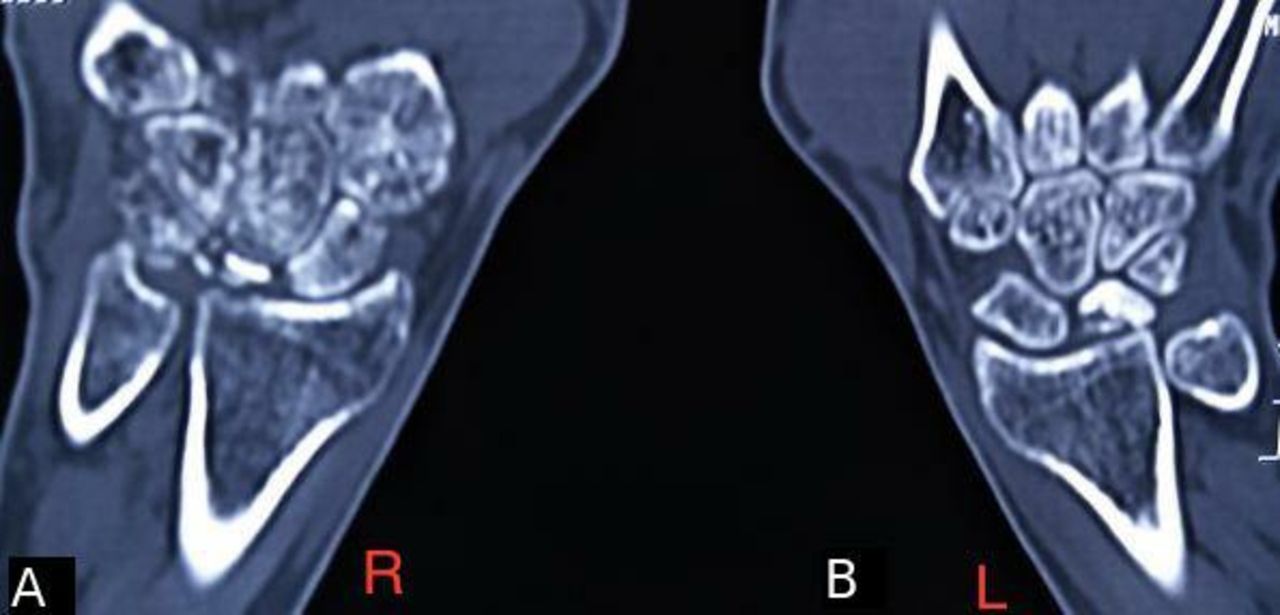
The laboratory analysis showed a total leucocyte count 9.86 ×109/L, rheumatoid factor 5 IU/mL, erythrocyte sedimentation rate 30 mm/h, C reactive protein 4 mg/L and serum uric acid 9.27 mg/dL. Radiographs were suggestive of Lichtman stage IIIB in the right wrist and staged IIIA Kienböck’s disease in the left wrist (figure 1). On CT scan, the lunate bone of the right side was significantly collapsed, sclerosed with multiple fragmentations with flexion of the scaphoid and the lunate bone of left side was partially collapsed and sclerotic with tiny cyst-like changes with deformed shape (figure 2). MRI revealed fragmentation and collapse of the lunate bone with diffuse-altered marrow signal intensity seen as heterogeneous low signal intensity on T1W images and heterogeneously hyperintense signal intensity on short tau inversion recovery (STIR) images (T2 weighted) in the right lunate bone. Rests of the carpal bones, distal end of radius and ulna have patchy marrow oedema in the form of STIR hyperintensities and hypointense signal on T1 weighted (complimentary CT sections show patchy osteopenia). Mild edematous changes are noted in the soft tissues over the dorsal aspect of the wrist (figure 3). The MRI of the left wrist showed partially collapsed and completely T1 hypointense with slight fragmentation and bone marrow oedema with areas of decreased signal intensity on T2-weighted images reflect sclerosis. Minimal soft tissue oedema was seen. The crystals were not visible in the MRI.

Preoperative posterior–anterior radiographs of bilateral wrist showing the complete collapse of lunate with multiple fragmentations, stage IIIB in the right wrist (A) and stage IIIA Kienböck’s disease in the left wrist (B).

Preoperative CT scans of the bilateral wrist. coronal sections of wrist showing the complete collapse of lunate with multiple fragmentations, stage IIIB in the right wrist (A) and stage IIIA Kienböck’s disease in the left wrist (B).
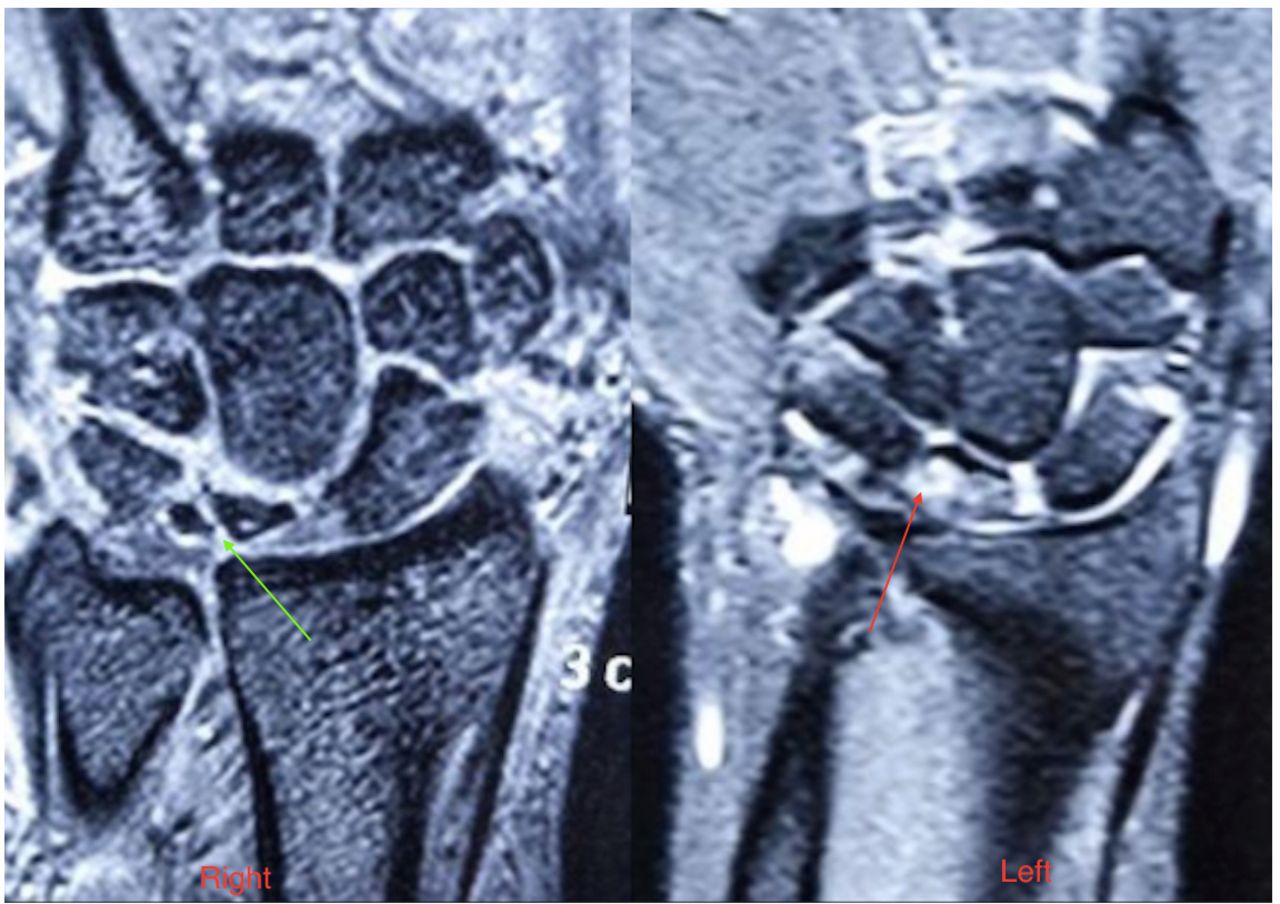
Coronal T2-weighted MRI of the bilateral wrist. The arrow (green) is indicating towards the fragmented, collapsed lunate of right side. The arrow (red) is indicating towards the collapsed lunate which shows oedema in T2-weighted images.
Differential diagnosis
The differential diagnosis was limited at the time of the presentation. Ulnar carpal impaction syndrome was excluded as wrist pain centred over dorsum in the absence of positive ulnar variance. Contusion or osteochondral injury was less likely as there was no history of trauma. Osteoid osteoma was less likely as there was no worsening of pain during nighttime. The CT appearance of the hyperdense sclerotic lesion in the absence of endosteal resorption and cortical thinning rules out the possibility of enchondromas. Therefore, based on the clinical features in the presence of negative ulnar variance, characteristic MRI and CT findings, the initial diagnosis of Kienböck’s disease and synovitis was made. Reactive synovitis was considered in response to necrosed bone and carpal instability. The final diagnosis of gouty synovitis concomitant with Kienböck’s disease was made after histopathological examination. Although patient had synovitis in setting of hyperuricemia, we did not consider gouty synovitis preoperatively because of the rarity of its combination with Kienbock’s disease. The final diagnosis was only made after biopsy report.
Treatment
The patient was explained about the different surgical options, which included proximal row carpectomy, lunate excision, and scapho–trapezio–trapezoid fusion, lunate excision, and scaphocapitate fusion, radial osteotomy and wrist fusion. As radiological features were suggestive of carpal collapse with compromised central column articulations and radioscaphoid articulation remains spared. Therefore, Lunate excision and scaphocapitate fusion were planned to bypasses the diseased central column after the detailed discussion with the patient. Open synovectomy was performed through the ligament sparing dorsal approach. Numerous crystal-like deposits were found during surgery. The lunate bone was excised. The biopsy sample was taken from lunate bone and synovial tissue and sent for histopathological examination. The cartilage of the scaphocapitate articulation was removed. The bone graft was harvested from the dorsal aspect of the distal radius. The bone graft was packed into the scaphocapitate articulation, and scaphocapitate articulation was fixed with two 2.5 mm compression screws (Arthrex). Wrist denervation was performed by neurectomy of the distal posterior interosseous nerve. Histopathological examination revealed multiple pale eosinophilic tophaceous deposits of various sizes within fibrocollagenous tissue that were negatively birefringent urate crystals under polarised light. Postoperatively, febuxostat 40 mg was started two times a day. Pain and swelling were significantly decreased in the postoperative period. The patient refused surgery over the left wrist as his pain decreased over the left side.
Outcome and follow-up
The postoperative pain after 1 week was 1.5, according to the visual analogue scale. The time to return to work was 5 months. At the end of 1 year, there was no recurrence of pain or swelling and no radiological sign of degeneration (figure 4). The Mayo wrist score was 70 points. The grip strength in the operated wrist was 58%, tip pinch was 48%, tripod pinch was 45% and key pinch was 61%. The range of motion flexion/extension arc was 10°/65°.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Posterior–anterior (PA) radiograph of the right wrist shows the fusion of scaphocapitate joint at a 1-year follow-up.
Discussion
Few cases of tophaceous involvement of wrist have been reported, and it can present as tendon ruptures, scapholunate dissociation, compressive median neuropathy and tenosynovitis.12–14 The proposed mechanism of avascular necrosis of lunate in gout may include crystal deposition in the cartilage and synovium or increased intra-articular pressure by joint effusion, which hampers vascular supply, and it leads to subsequent disintegration.15 All three reported cases of Kienböck’s disease with gout were unilateral. The first case was reported in a 42-year-old left-handed labourer who had a prior history of acute attacks of ankle monoarthritis in the setting of hyperuricemia (11 mg/100 mL).7 A case of stage II Kienböck’s disease was reported in a 54-year-old male patient who had a history of an acute attack of gout in greater toe 5 years before presentation.8 Arthroscopic synovectomy and partial wrist denervation were performed. Recently, another case was reported, who had stage IIIB Kienböck’s disease with a normal uric acid level in a 49-year-old patient.9 There was no prior history of gout in any joint. Arthroscopic synovectomy was performed. The patient in our study had hyperuricemia with no history of polyarthralgia, first MTP joint involvement, or tophi deposits anywhere in the body. Intraoperative findings and subsequent histopathological confirmation of tophi in the synovium made the diagnosis. The previous two case reports advocated different surgical approaches for Kienböck’s disease with gout.8 9 Synovectomy was done as a single procedure for stage II Kienböck’s disease, and IIIB Kienböck’s disease rather than revascularisation procedure or wrist fusion. There was a partial collapse in the lunate and a decrease in carpal height. We noticed a complete collapse of the lunate with multiple fragmentations. So lunate excision with scaphocapitate fusion was combined with synovectomy procedure. The previous reports emphasised that the suspicion of Kienböck’s disease should be considered in gout patients. However, they did not recommend radiograph or MRI screening of contralateral wrist to rule out preclinical stages of avascular necrosis. There are few case reports of bilateral Kienböck’s disease reported in the literature. In a study of 251 Kienböck’s disease patients by Yazaki et al, 11 patients were found to be bilaterally involved.10 They did not find any systemic risk factors, such as steroids or systemic lupus erythematosus (SLE), as opposed to unilateral disease. Unlike femoral head osteonecrosis, there are no apparent risk factors defined for bilateral Kienböck’s disease due to the rarity of its involvement in systemic diseases. However, there are few reports of bilateral Kienböck’s disease in SLE,2 scleroderma4 and Legg-Calvé-Perthes disease.16 The present case of bilateral Kienböck’s disease combination with gout in the absence of ulnar-negative variance indicates a relationship between them. However, the literature fails to give any association between gout and Kienböck’s disease due to its rarity of combination.
Learning points
Gout is a systemic disease and can also cause bilateral osteonecrosis of lunate.
Serum uric acid levels should be done in patients of Keinbock’s diease.
Suspicion of contralateral wrist involvement should be sought in cases of symptomatic unilateral disease.
Footnotes
Contributors DC wrote the manuscript and provided clinical photographs. VS drafted and revised the manuscript. MTA drafted and wrote the manuscript. MTA performed the surgery. All authors have contributed significantly to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.