Article Text

Statistics from Altmetric.com
Description
A 68-year-old man with no significant medical history was brought to the emergency department for an episode of syncope after exertion. He regained consciousness before arrival in the hospital. He reported some shortness of breath in the emergency room but denied any chest pain. In the emergency room, his heart rate was 98 beats/min, blood pressure 136/82 mm Hg and O2 saturation 93% on room air. His high-sensitivity troponin was 123 (<14 ng/L), brain natriuretic peptide was 870 pg/ mL (<100 pg/mL) D-dimer was 2280 (<500 ng/mL) and ECG showed normal sinus rhythm with right bundle branch block and non-specific ST-segment and T-wave changes. CT angiogram of the chest demonstrated extensive bilateral pulmonary emboli with evidence of right ventricular (RV) dilatation and slight bowing of the interventricular septum towards the left. A point of care echocardiogram showed moderate right-sided cardiac chamber enlargement and reduced right ventricular contractility with apical sparing (McConnell’s sign). RV systolic pressure was noted to be 43 mm Hg (15–25 mm Hg) (figure 1 and video 1).

{kind=link}
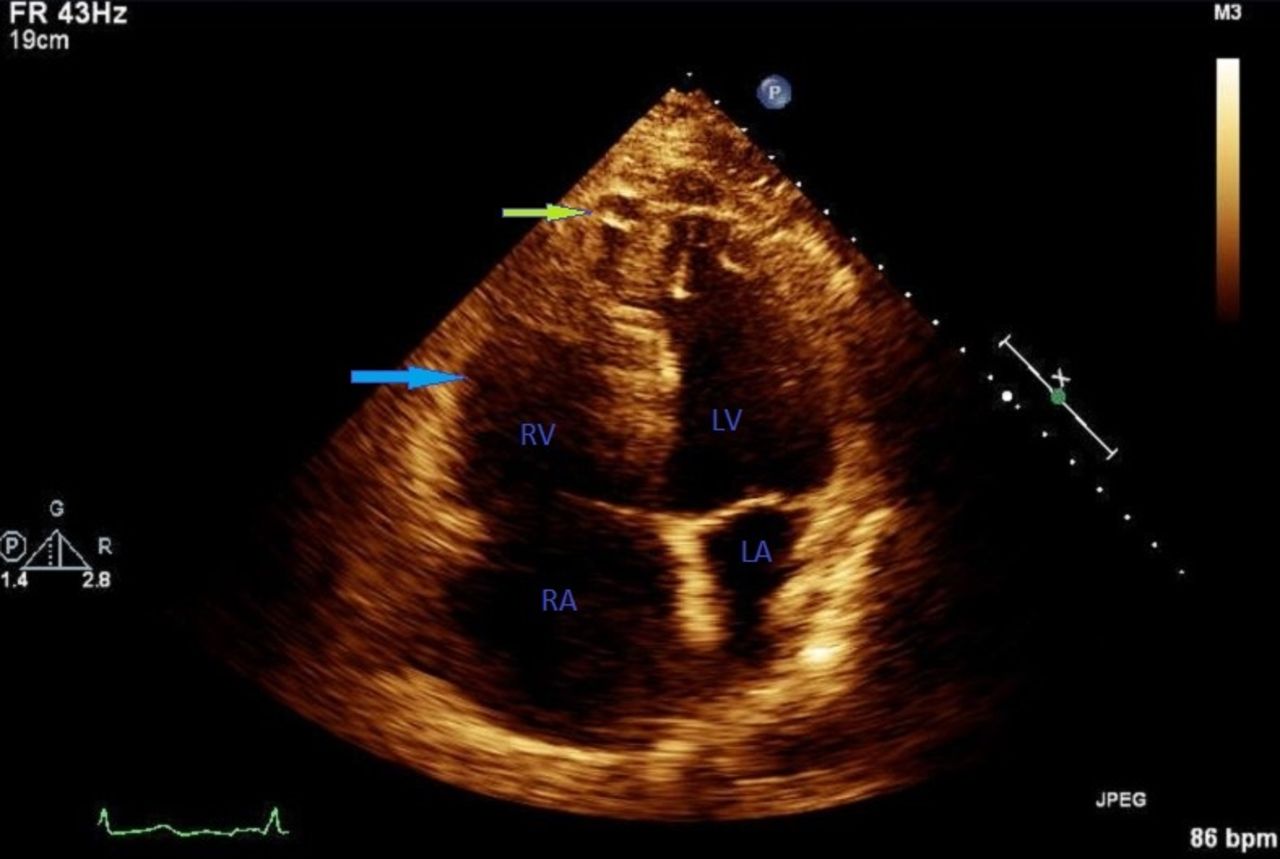
Image of echocardiogram during systole showing contraction of the apex of the RV (green arrow). LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
He was admitted to the intensive care unit and initially started on heparin infusion followed by catheter-directed thrombolysis with tissue plasminogen activator (TPA). After obtaining consent, he was taken to the catheter laboratory, a 6-French pigtail catheter was placed into the main pulmonary artery for pulmonary artery angiogram. Two 90 cm Unifuse perfusion catheters were selectively placed into the right and left pulmonary arteries. Each infusion catheter was placed to continuous TPA infusion for selective thrombolysis. TPA was initiated at 0.5 mg/hour in each catheter to a total of 1 mg/hour for a duration of 24 hours. Follow-up angiogram demonstrated that the right pulmonary artery was entirely clear with 1 cm residual defect in the left upper branch. The patient was eventually transitioned to novel oral anticoagulant and discharged home. A follow-up echocardiogram done 20 days after catheter-directed thrombolysis showed normal RV size and contractility.
Pulmonary embolism affects 225 000 Americans and 300 000 Europeans each year. It is the third leading cause of cardiovascular mortality in North America.1 Acute RV failure constitutes high mortality in pulmonary embolism and early identification and treatment can potentially reverse RV failure.2
Echocardiography remains useful in identifying RV strain and helps justify the use of thrombolytic therapy in patients with massive acute pulmonary embolism.3 4 McConnell et al were the first to describe the localised pattern of dyskinesia that affects the middle free wall of the RV.5 Though it lacks sensitivity, it remains a highly specific and useful sign of acute pulmonary embolism.6
Learning points
Transthoracic echocardiogram remains a valuable imaging modality to assess right ventricular strain in patients with acute pulmonary embolism.
Availability and use of bedside/point of care echocardiography can aid in the rapid diagnosis of impending haemodynamic compromise and maybe a life-saving measure.
McConnell sign is highly specific in cases of acute massive pulmonary embolism and when present can aid in decision making to start thrombolytic therapy in the right clinical settings.
Footnotes
Contributors AA and RB: literature search, research, data acquisition and interpretation and drafting of manuscript. SP: proofreading, final drafting of the manuscript, corresponding author.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.