Article Text

Statistics from Altmetric.com
Description
A 69-year-old man presented with a 2-week history of constipation and severe intermittent periumbilical pain. He also described loss of appetite and 6 kg loss of weight over the 2-week period. He presented twice to his general practitioner over these 2 weeks, who initially prescribed laxatives for constipation then referred him to the emergency department for ongoing pain. A colonoscopy had been done 9 years earlier for constipation and the patient reported it as unremarkable. He had a family history significant for bowel cancer in a first-degree relative and was a smoker. He was haemodynamically stable with a tender mass in the right upper quadrant on examination.
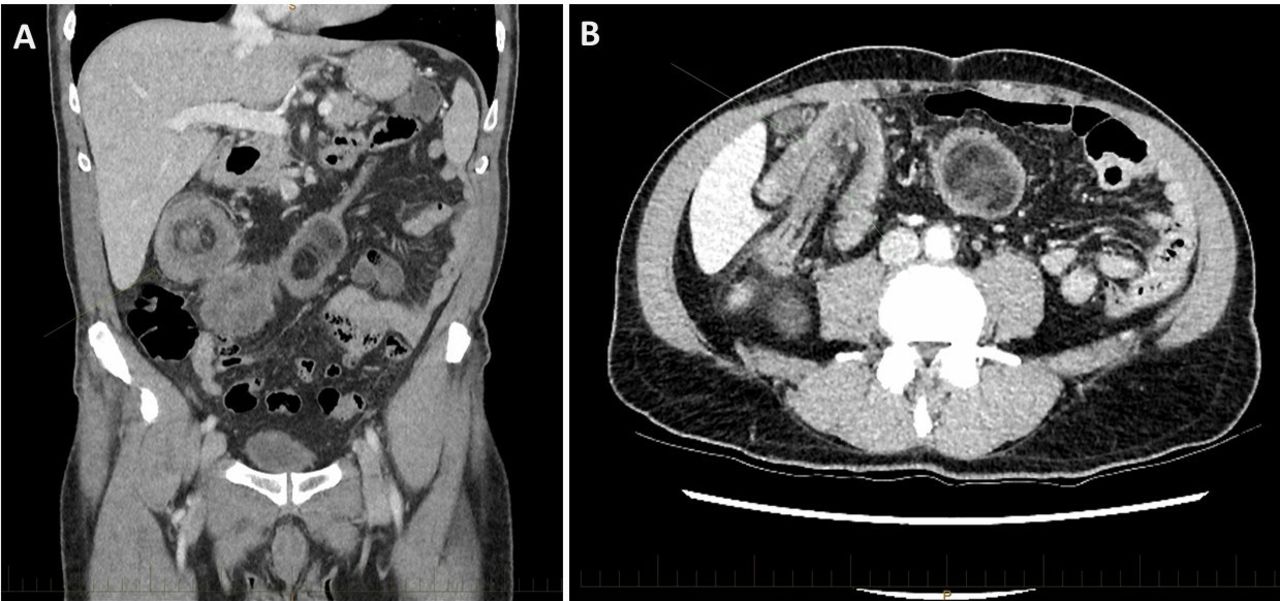
The patient subsequently had an abdominal CT scan, which revealed a large bowel intussusception of the hepatic flexure into the transverse colon, with a low-density heterogenous soft-tissue mass as the lead point (figure 1A,B) and no features of large bowel obstruction. His blood results showed a raised C reactive protein (CRP) of 120 but were otherwise unremarkable.

CT of the abdomen showing classical imaging features (A) coronal plane with target sign and (B) axial plane with sausage-shaped telescoping of hepatic flexure into the transverse colon.
He underwent an emergency laparoscopic-assisted right hemicolectomy, revealing a 6.0×3.5 cm polypoid submucosal lesion with surrounding tattoo ink in the large bowel lumen with necrotic changes at the tip and otherwise macroscopically normal large bowel mucosa (figure 2). Histopathology confirmed a lipoma with fat necrosis and ischaemic changes but no suspicious features for malignancy. We later correlated this result with his original colonoscopy, which reported a large submucosal mass that was tattooed at the time and biopsies confirming a lipoma. He had an uncomplicated postoperative recovery.

{kind=link}
{kind=link}
Macroscopic photograph of the specimen showing 6.0×3.5 cm submucosal lipoma with ischaemic necrosis overlying the tip.
Intussusception is the the most common cause of acute small bowel obstruction in children aged <3 years but comprises only 1% of adult bowel obstruction presentations.1 Additionally, in the adult population, a pathological lead point is often identifiable, whereas a minority of paediatric intussusceptions present with a lead point. Of the 1% adult intussusception, malignancy forms the majority of lead point aetiology (65%–70%).1 The lead point is pulled forward by normal peristalsis, telescoping or prolapsing the affected segment of bowel (intussusceptum) into another segment of bowel (intussuscipiens). A lipoma is a rare cause of adult intussusception but has been documented in cases worldwide.2 This report describes a case of a late presentation of an adult intussusception due to a lipoma with classical imaging findings and intraoperative photographs of the lesion. The role of elective bowel resection in patients with large submucosal lipomas should be considered to prevent future complications.
Learning points
Large bowel intussusception is rare in adults and is usually due to a malignant lead point.
The classic imaging features are the ‘target’ sign and a sausage-shaped mass.
Consider the role of elective bowel resection in patients with large submucosal lipomas to prevent future complications.
Footnotes
Contributors TS conceived the project, executed the case write-up and produced the images. MW performed the literature review and contributed to the case write-up. JC edited the final document for submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.