Article Text

Statistics from Altmetric.com
Description
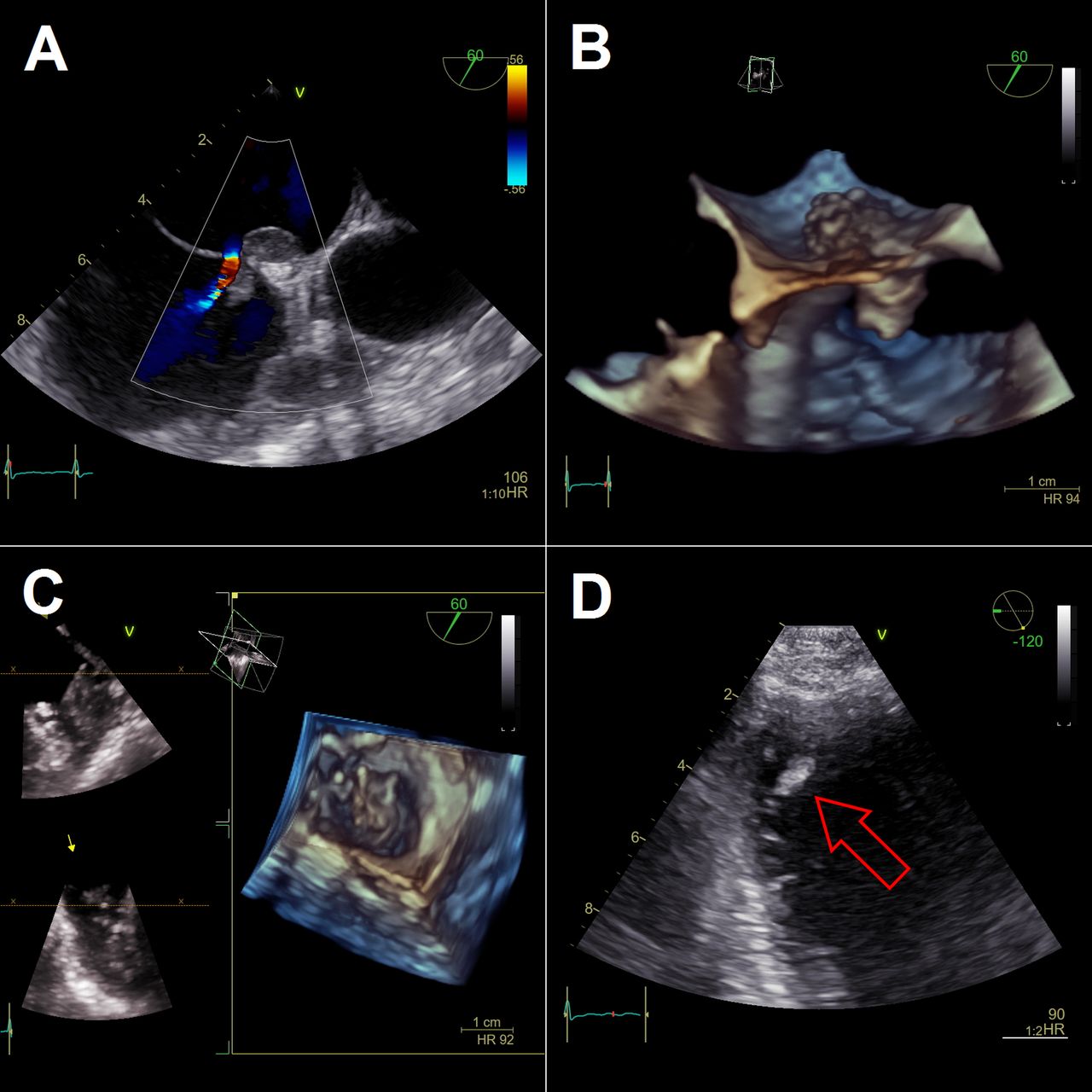
A 58-year-old woman with new onset atrial fibrillation with rapid ventricular response (heart rate (HR) 161 bpm) and acute decompensated heart failure of unknown aetiology was admitted to our emergency department. Anticoagulation with unfractionated heparin was started immediately and transoesophageal echocardiography (TOE) to rule out left atrium and left atrial appendage (LAA) thrombus before early electrical cardioversion was performed.1 2 TOE showed a thrombus ‘in transit’ in an atrial septal defect (ASD) with left to right shunt (figure 1A,B, videos 1 and 2), and a large thrombus in the LAA (figure 1C, video 3). Additional transthoracic echocardiography showed severely reduced left ventricular (LV) ejection fraction of 25%–30% and a third intracardiac thrombus in the apex of the left ventricle (figure 1D, arrow; video 4). Thus, cardioversion was contraindicated due to a haemodynamically stable situation1 3 and medical treatment for rate control of atrial fibrillation along with medical treatment of heart failure was established. Since no guideline recommendations or even case reports on the optimal anticoagulation management of triple intracardiac thrombus exist, empirical anticoagulation with unfractionated heparin was continued and switched to apixaban 14 days later after complete resolution of the LV and ASD thrombus. Screening for various coagulopathies (factor V Leiden mutation, prothrombin mutation G20210A, protein C deficiency, protein S deficiency, antiphospholipid syndrome, antithrombin deficiency), drug-induced thrombophilia and for solid and haematological malignancies was negative. Follow-up 2 months later showed complete recovery of systolic LV function, stable sinus rhythm and no evidence of residual intracardiac thrombus.

{kind=link}
Transoesophageal echocardiography (TOE) colour doppler mode (A) and three-dimensional mode (B) of the interatrial septum showing a thrombus ‘in transit’ in an atrial septal defect with left to right shunt. TOE three-dimensional mode depicting a large thrombus in the left atrial appendage (C) and transthoracic echocardiography showing a thrombus in the apex of the left ventricle (D, arrow). HR, heart rate.
Learning points
In atrial fibrillation of unknown duration without established anticoagulation left atrium and left atrial appendage (LAA) thrombus must be excluded by transoesophageal echocardiography before early cardioversion.
If left atrium or LAA thrombus is found in atrial fibrillation, immediate cardioversion in haemodynamically stable situations should not be done but anticoagulation therapy with repeated imaging is indicated.
The optimal anticoagulation therapy in multilocular intracardiac thrombus is not known, empirical anticoagulation with unfractionated heparin and apixaban showed complete resolution of multilocular intracardiac thrombus in our case.
Footnotes
Contributors NK and KW drafted the manuscript, SAM corrected and completed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.