Article Text

Statistics from Altmetric.com
Description
A 19-year-old man presented at the emergency department with asthenia and anorexia for 2 weeks, associated with nonspecific abdominal pain. The patient reported diarrhoea for the last 6 days, without blood neither mucus. The physical examination showed signs of dehydration (dry mucous membranes) and the abdomen was soft and depressible, with diffuse discomfort on palpation. A slightly granular texture was noted on digital rectal examination.
The abdominal ultrasound showed a hypoechogenic mass in the right hypochondrium, corresponding to a colo-colonic intussusception on CT, associated with multiple polyps throughout the whole colon (figure 1A–D). These polyps were confirmed by colonoscopy performed 15 hours after the CT, showing a larger polyp located in the ascending colon (hepatic angle), corresponding to the location of the intussusception detected previously, that was no longer present. The pathological study of two polyps diagnosed tubulovillous adenomas and the genetic study revealed a mutation in the APC gene, compatible with Familial Adenomatous Polyposis (FAP). The patient has undergone prophylactic proctocolectomy and the surgical specimen showed multiple adenomas throughout the colon, with millimetre dimensions. A larger polyp with 30 mm was confirmed in the ascending colon, which had low-grade dysplasia (figure 2A–D).

(A-B) Contrast-enhanced CT scan shows the colo-colonic intussusception with bowel-within-bowel configuration (outer intussuscipiens and central intussusceptum), demonstrated by the typical “sausage-shaped” image in the axial plane (arrow in A) and “target-like” image in the coronal plane (arrow in B). It is possible to identify the distinct invaginated structures, including the entering wall, returning wall and mesenteric fat and vessels (asterisk in A). Note the multiple polyps throughout the mucosal surface of the colon. (C–D) There are countless polyps covering the rectum and transverse colon.

{kind=link}
{kind=link}
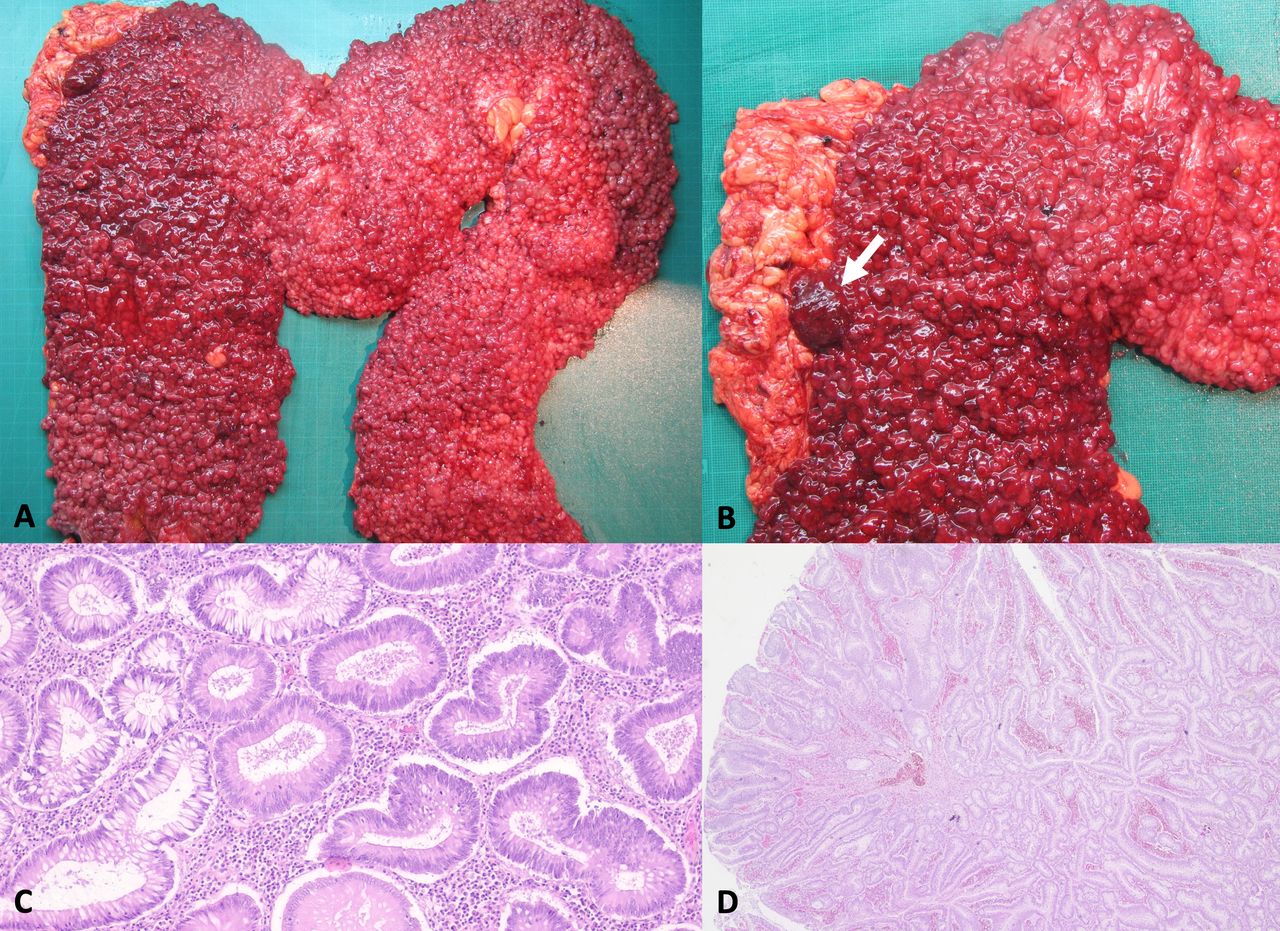
(A-B) Proctocolectomy specimen revealing multiple polyps covering the entire mucosal surface of the colon. A biggest polyp in the ascending colon of about 30 mm stands out (arrow in B). (C) Histology (H&E 20x): the larger polypoid lesion corresponds to a tubular adenoma with low grade dysplasia. (D) Histology (H&E 100x): one of the adenomatous polyps from the left colon, with low and high grade dysplasia.
FAP is an inherited autosomal dominant disease, caused by germline mutations of the APC gene (chromosome 5q21), corresponding to the development of hundreds to thousands of adenomas throughout the colon and rectum. It occurs with a frequency of 1 in 10 000 individuals.1–3
The polyps appear at the second decade of life, with a mean age of 15 years.3 If the patients are left untreated, they almost inevitably develop colorectal cancer (CRC) by the age of 35–40 years.4
This case report describes a patient with FAP, with a spontaneous mutation – index case – associated with the occurrence of a colo-colonic intussusception. To the best of our knowledge, there are no previously published reports addressing the association between FAP and colo-colonic intussusception.
Intussusception is the invagination of a bowel loop with its mesenteric fold (intussusceptum) into the lumen of a contiguous portion of bowel (intussuscipiens). Adult intussusception is uncommon and the majority of the cases result from changes in the normal peristalsis due an underlying lesion that acts as a lead point.5 6
The adenomas in FAP are almost all less than 5 mm in diameter and less than 1% of polyps are larger than 10 mm, likely being too small to become a leading point of an intussusception.7 This raises the curiosity for the present case, because a polyp with an uncommon size (30 mm) was disclosed in the same location of the intussusception detected at CT (figure 2B), suggesting to be the leading point of the transient intussusception.
The CT imaging findings are virtually pathognomonic for diagnosing intussusceptions in adults, corresponding to the presence of an outer intussuscipiens and central intussusceptum, with identification of the distinct anatomic features (figure 1A).8 9
The patient will undergo a surveillance programme by endoscopic studies, addressing the risk of other gastrointestinal tract tumours, and a periodic examination of the ileostomy.2 3
Patient’s perspective
I am glad that my case can help the scientific community to better understand my disease and benefits other patients who find themselves in similar situations.
Learning points
Exceptionally the polyps of FAP may be large enough to cause intussusception, a rather unusual manifestation of this condition.
The clinical presentation of intussusception in adults can be nonspecific, making CT pivotal for the diagnosis.
The prophylactic surgical treatment is critical for preventing development of CRC in FAP.
Footnotes
Contributors PGO conceived and designed the case report. RA and CF collected and interpreted patient data. PGO and CF collaborated in bibliographic research and prepared the manuscript draft with important intellectual input from LCS. All authors approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.