Article Text

Statistics from Altmetric.com
Description
A 32-year-old woman, known case of chronic myeloid leukaemia on chemotherapy, presented with acute onset of bilateral foot pain and paraesthesia. On examinations, the pedal pulses were absent bilaterally with reduced cutaneous temperatures over the ankles and feet. Lower limb arterial Doppler examination revealed the absence of colour flow in the distal parts of bilateral anterior and posterior tibial arteries. Interestingly, bilateral common femoral arteries and the superficial femoral arteries (SFA) appeared uniformly small in calibre.
An immediate magnetic resonance angiography was performed, which revealed presence of bilateral complete persistent sciatic arteries (PSA) with small calibre/hypoplastic bilateral SFAs having no continuity with the respective popliteal arteries. Distal thrombotic occlusion of bilateral anterior and posterior tibial arteries was observed (figures 1 and 2). No significant stenosis was seen in the abdominal aorta, iliac or popliteal arteries. The patient was started on intravenous heparin following which there was significant resolution in symptoms. Follow-up Doppler examination after 2 weeks showed complete recanalisation of the distal tibial arteries.

Maximum intensity projection images of magnetic resonance angiography (A–C) reveals the presence of bilateral complete persistent sciatic arteries (PSA) with hypoplastic bilateral superficial femoral arteries (SFA) having no continuity with the respective popliteal arteries. Distal thrombotic occlusion of bilateral anterior and posterior tibial arteries is also present.
{kind=link}
{kind=link}
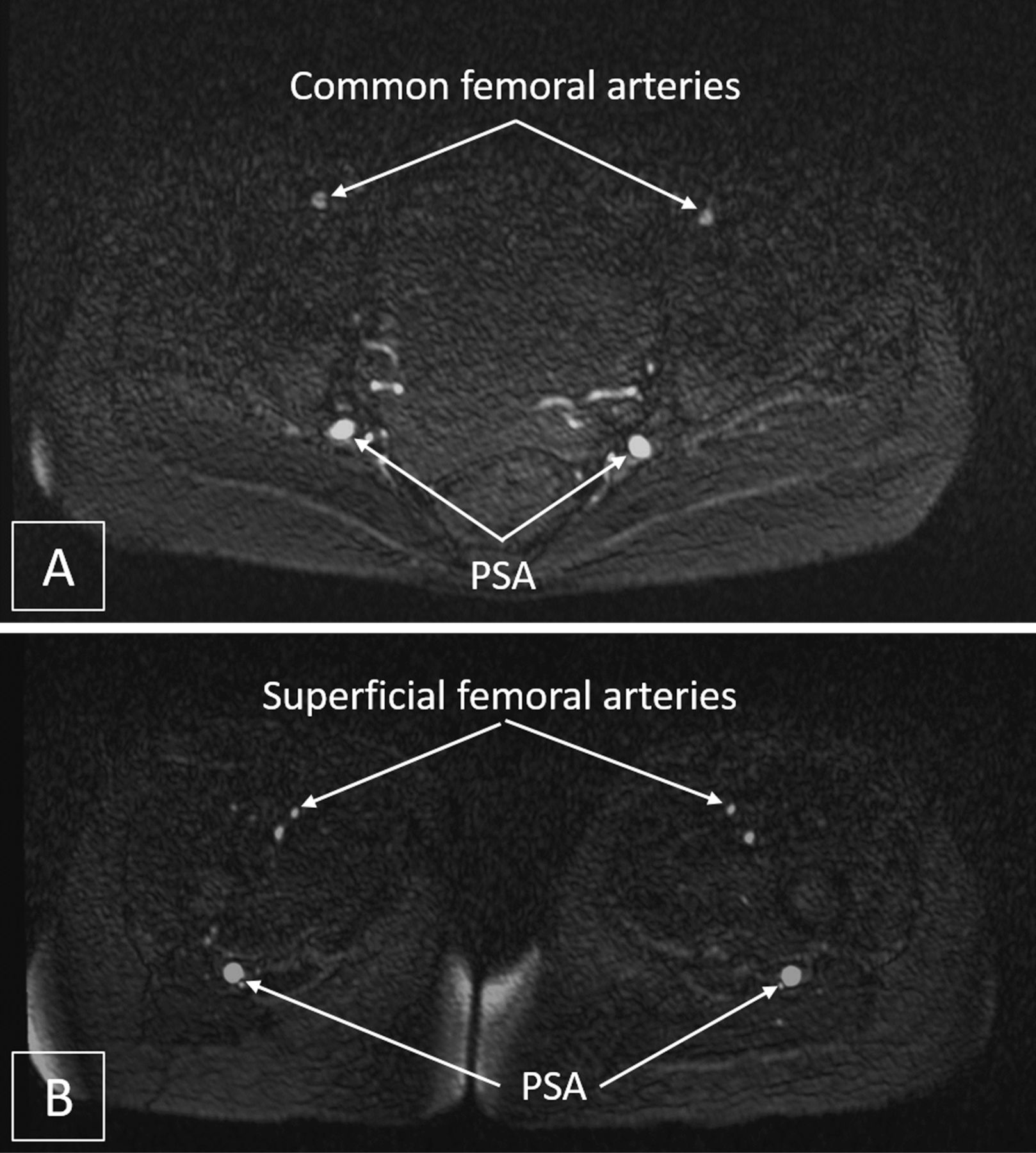
Axial magnetic resonance angiography images at the level of groin (A) and upper thigh (B) reveals the presence of bilateral complete persistent sciatic arteries (PSA) with hypoplastic bilateral common and superficial femoral arteries (SFA).
PSA is a rare arterial embryologic anomaly reported in 0.03%–0.06% of the population and represents failure of regression of the embryonic sciatic artery, which is a branch of the umbilical artery and the principal arterial supply of the developing lower limb.1 Most of the cases have unilateral anomaly with bilateral PSAs representing only about 30% of all cases.
Complete PSA (where it is the main blood supply to the lower limb or popliteal and infrapopliteal branches) is much more common than incomplete. In the presence of a complete PSA, the SFA may be normal (type 1), incomplete (type 2a) or absent (type 2b). In the presence of incomplete PSA (types 3 and 4), the femoral arteries are normally developed.2 Though PSAs are prone to early atheromatous degeneration and aneurysm formation, most often they are asymptomatic. The etiologies associated with a symptomatic PSA are aneurysm, PSA occlusion, PSA stenosis and distal occlusions, in decreasing order of frequency. In cases of isolated symptomatic distal occlusions, a trial of thrombolysis/anticoagulation can be therapeutic, while other etiologies may require various combinations of medical, surgical and endovascular approaches.
Learning points
Persistent sciatic artery (PSA) is a rare arterial embryologic anomaly representing failure of regression of the embryonic sciatic artery, which is the principal arterial supply of the developing lower limb.
Most cases are unilateral with bilateral PSAs representing less than one-third of all the cases.
Though PSAs are prone to early atheromatous degeneration and aneurysm formation, most often they are asymptomatic.
Footnotes
Twitter @rengadr
Contributors MS, NNP, RR and PJ have participated sufficiently in the conception of the idea, the development of the intellectual content, design and writing and the final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.