Article Text

Statistics from Altmetric.com
Description
A 12-year-old girl presented with a painful, non-pulsatile swelling in the right supraclavicular fossa of 6-month duration, which increased in size on straining and coughing (figure 1A). Physical examination and auscultation confirmed the non-pulsatile nature of the swelling with absence of any thrill or bruit. A Doppler ultrasound examination (figure 1B) and a subsequent contrast-enhanced CT (figure 1C–D) confirmed the swelling to be an outpouching, measuring 3.3×3×2.5 cm, arising from the posteromedial aspect of the right external jugular vein (EJV). No other venous channels were seen communicating with the lesion. The right EJV was seen to be displaced laterally and draped over the swelling. Thin septations were also seen within the lesion. No thrombus was seen.

Clinical photograph (A) reveals a 3×3 cm swelling (delineated by arrows) in the right supraclavicular fossa. Ultrasound Doppler image (B) shows venous flow within the sac. Contrast-enhanced CT images in the axial (C) and oblique coronal (D) planes demonstrate an outpouching (*), measuring 3.3×3×2.5 cm, arising from the posteromedial aspect of the right external jugular vein (EJV), which is seen to be displaced laterally and draping over the swelling. Thin septations (thin white arrows) are also seen within the lesion with no thrombus present.
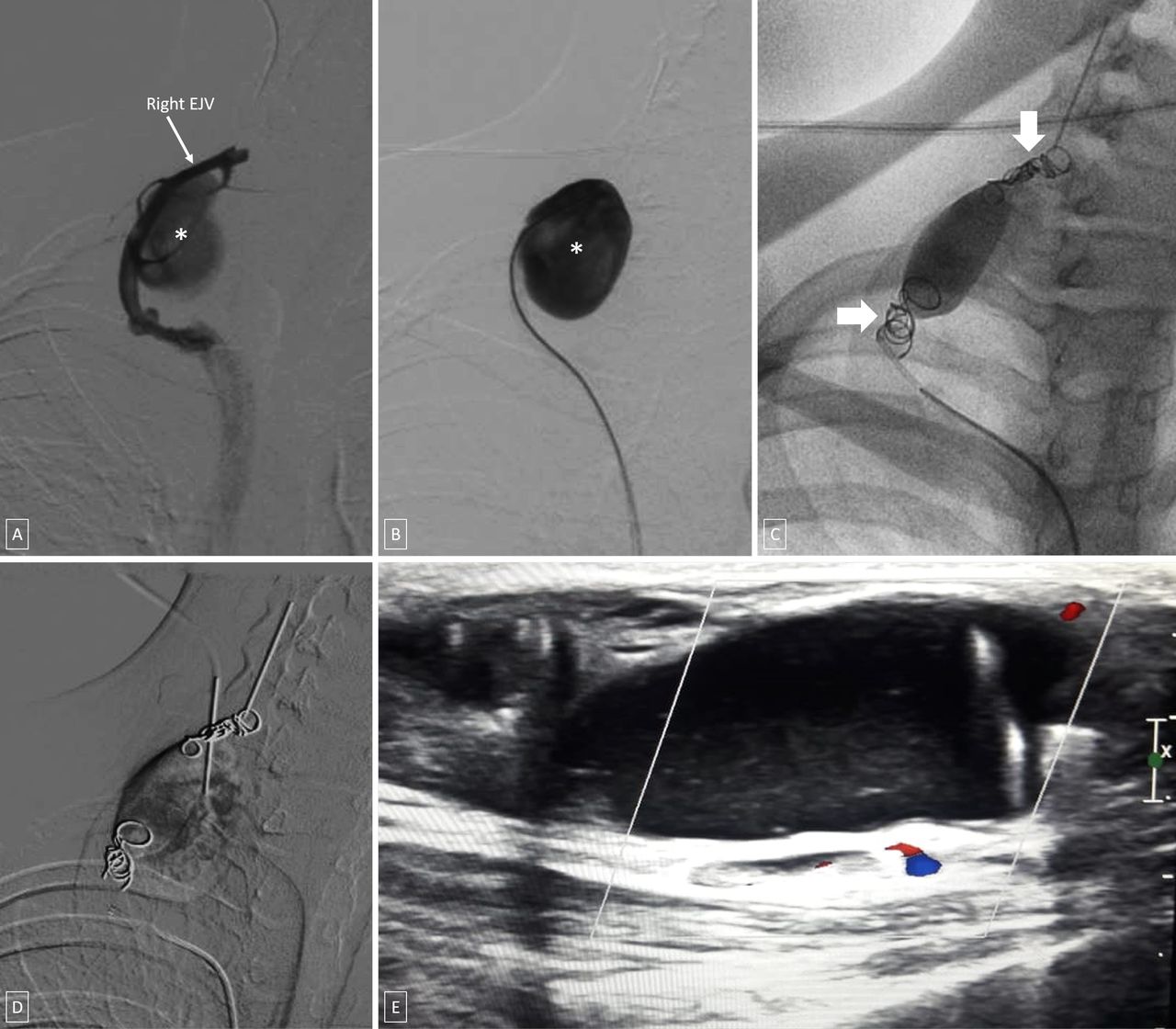
In view of persistent pain and for cosmetic reasons, the patient was planned for endovascular embolisation. The right EJV was cannulated proximal to the outpouching using a butterfly cannula (22G) and diagnostic venogram performed which showed the presence of a well-defined, multi-septated, saccular outpouching from its posteromedial aspect with a narrow neck (figure 2A–B). The right EJV was cannulated via a right transfemoral venous access and successfully embolised, both proximal and distal to the neck of outpouching, using multiple pushable coils (figure 2C). The sac was then punctured percutaneously, aspirated and a contrast injection done to confirm absence of any tributaries or any reflux into the right EJV. Subsequently, foam-sclerosant (3 mL of 1% polidocanol mixed with air in 1:4 ratio) was injected into the sac and compressed (figure 2D). Ultrasound Doppler showed complete thrombosis of the sac (figure 2E) along with reduction in the size of the swelling at 2-week follow-up examination.

{kind=link}
{kind=link}
Diagnostic venogram (A, B) reveals a well-defined, multi-septated, saccular outpouching (*) from its posteromedial aspect with a narrow neck. (C) The right external jugular vein (EJV) embolised both proximal and distal to the neck of outpouching using multiple coils (thick arrows). (D) Percutaneous injection of foam-sclerosant into the sac. Ultrasound Doppler (E) reveals complete thrombosis of the sac with no colour flow within.
EJV aneurysm is an exceedingly rare entity and hence their exact incidence is unknown. They typically present as a cervical mass, which shows alteration in size with position and with Valsalva manoeuvre. While clinical findings and ultrasound is often diagnostic, CT can help provide a roadmap for retrograde venous catheterisation of the feeding vein, demonstrate any additional feeders and delineate deeper extensions of the venous aneurysm, which might be overlooked on the ultrasound examination. Patients may present will dull pain at the site of swelling, but are mostly asymptomatic. Usually, they do not undergo significant change in size or morphology over time and hence can be followed up without intervention. Management is commonly indicated for cosmetic reasons or when complications such as thromboembolism, rupture or thrombophlebitis arise.1 While majority of the previously reported cases have been managed with surgical excision, endovascular treatment may be an attractive option as it circumvents the issues and complications of surgery such as need for anaesthesia, potential injury to surrounding structures, wound infection, haemorrhage and scar.2 However, it would be prudent to note that secondary to the scarcity of available literature, no specific guidelines for the treatment of these lesions exist.
Learning points
External jugular vein aneurysm is an exceedingly rare entity and their exact incidence is unknown. As commonly they do not undergo significant change in size or morphology, they can be followed up without intervention.
Management is indicated for cosmetic reasons or when complications such as thromboembolism, rupture or thrombophlebitis arise.
It can be managed by both surgical and endovascular approaches; however, no specific guidelines for the treatment of these lesions exist.
Footnotes
Contributors NNP participated sufficiently in the conception of the idea, development of the intellectual content, design, writing and final approval of the manuscript. MS participated sufficiently in the conception of the idea, development of the intellectual content, design, writing and final approval of the manuscript. AD participated sufficiently in the conception of the idea, development of the intellectual content, design, writing and final approval of the manuscript. SK participated sufficiently in the conception of the idea, development of the intellectual content, design, writing and final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.