Article Text

Statistics from Altmetric.com
Description
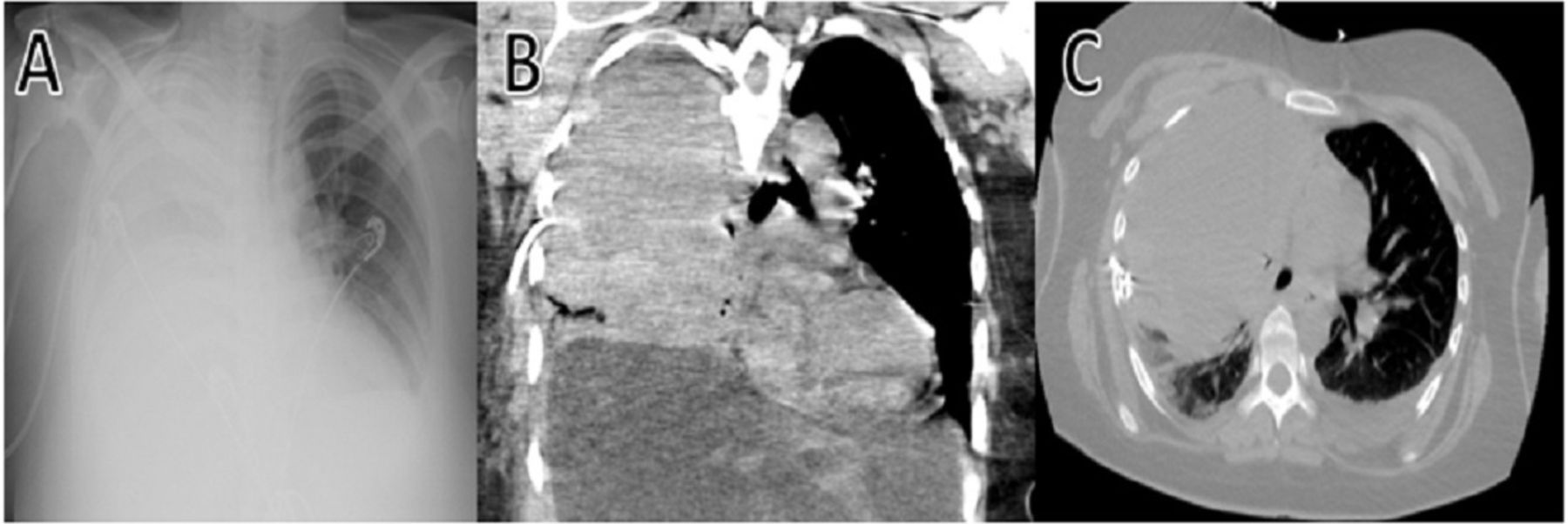
A 68-year-old woman presented to the emergency room with ongoing fevers, dyspnoea and pleuritic chest pain. She was recently discharged about a week ago for multifocal pneumonia. Her medical history was significant for atrial fibrillation. She was on warfarin for anticoagulation but had not been taking it for 5 days due to her illness. Her complete blood count and coagulation panel were within normal limits with an international normalised ratio of 1.3. On initial evaluation, chest radiograph (CXR), shown in figure 1A and chest CT, shown in figure 1B and C, demonstrated a moderate right-sided pleural effusion that appeared loculated with a right lower lobe opacification concerning for compressive atelectasis versus consolidation (figure 1). The lung infiltrates from previous pneumonia had improved, but the right-sided pleural effusion was new. A CT-guided pigtail catheter was placed that drained 450 mL of serosanguinous fluid from the right-sided pleural effusion. Follow-up CXR (figure 2A) and CT chest (figure 2B) post-drainage showed improved pleural effusion. Still, a small loculated pleural effusion remained despite the well-positioned pigtail catheter within the vicinity of the pleural fluid pocket. Pleural fluid results revealed a neutrophil-predominant exudative effusion. The decision was made to medically treat her loculated effusion by starting intrapleural enzymes of tissue plasminogen activator (tPA) involving 10 mg alteplase, and 5 mg dornase alfa (DNase) two times per day for the next 3 days. Blood and pleural fluid culture returned negative for micro-organisms. While receiving intrapleural tPA, her warfarin was held and substituted with deep venous thrombosis (DVT) prophylaxis. As she remained stable clinically during her hospital course, repeat chest imaging was not performed. Her chest tube continued to drain 100–150 mL of serosanguinous pleural fluid daily for the next three consecutive days. However, on the fourth day of hospitalisation, she developed worsening hypoxic respiratory failure and right-sided chest pain. Her repeat haemoglobin was 9 g/dL, which significantly decreased from 12.5 g/dL obtained the day prior that resulted in immediate cessation of DVT prophylaxis. Of note, her admission haemoglobin was 13 g/dL. Her pleural fluid drainage was minimal at 50 mL over 24 hours and appeared sanguineous. Repeat CXR (figure 3A) and CT chest (figure 3B and C) demonstrated complete opacification ‘white-out’ of right lung field with large heterogenous attenuating pleural fluid collection occupying right lung field suggestive for haemothorax with mediastinal shift to the left and compressive atelectasis of right middle and lower lobe. She was taken urgently to the operating room for right chest thoracotomy and complete decortication that confirmed the diagnosis of haemothorax likely secondary to the use of intrapleural tPA and DNase.

CXR (A), CT chest lung window (B) and mediastinal window (C) demonstrating moderate right-sided pleural effusion that appears loculated with a right lower lobe opacification concerning for compressive atelectasis versus consolidation. CXR, chest radiograph.

CXR (A) and CT chest (B) revealed the location of CT-guided pigtail catheter placement within the vicinity of loculated right-sided pleural effusion. CXR, chest radiograph.
{kind=link}
{kind=link}
{kind=link}
CXR (A) and CT chest (B and C) demonstrated complete opacification ‘white-out’ of right lung field with large heterogenous attenuating pleural fluid collection occupying the right lung field concerning for haemothorax with mediastinal shift to the left and compressive atelectasis of right middle and lower lobe. CXR, chest radiograph.
Intrapleural fibrinolytic therapy using tPA alone or with DNase, streptokinase or urokinase has been used as an alternative to surgical treatment of loculated pleural effusions with failed drainage. The First Multicenter Intrapleural Sepsis Trial (MIST-1) trial randomised patients with parapneumonic effusion to receive either intrapleural fibrinolytic therapy or placebo with no improvement in clinical outcomes involving length of hospitalisation or the requirement for surgical intervention.1 The follow-up MIST-2 trial randomised patients to receive either intrapleural tPA or DNase alone or in combination where radiographic improvement in pleural effusion, reduction in the length of hospitalisation and the need for surgical intervention were noted in the combination group.2 In the MIST-2 trial, all severe intrathoracic bleeding occurred in the tPA/DNase combination group. Several observational studies have demonstrated that the risk of developing haemothorax is highly variable, ranging between 1.8% and 10% in patients receiving intrapleural tPA with/without DNase.2–4 However, the risk increases exponentially to 28%–33% with the concurrent administration of therapeutic anticoagulation or when a higher dose of intrapleural tPA (20 mg alteplase) was used, regardless of coagulation panel results.3 5 The risk of bleeding was not increased in patients receiving aspirin, clopidogrel or prophylactic subcutaneous heparin.5 Interestingly, there is a case report in which a patient experienced severe intrapleural bleeding with opacification of a hemithorax after receiving intrapleural tPA/DNase while fully anticoagulated.6 This suggests that bleeding risk may be increased using this combination. Our case suggests but does not prove that similar complications can occur during intrapleural tPA/DNase administration when DVT prophylaxis with an anticoagulant is used. There is currently no consensus on whether anticoagulation is a contraindication to intrapleural enzymes. There are relatively few studies devoted to the association between intrapleural fibrinolytic therapy and haemothorax. While most are small series or case reports, our case demonstrates that haemothorax requiring surgical intervention can occur with the use of intrapleural tPA and DNase.
Learning points
Intrapleural tissue plasminogen activator (tPA)/dornase alfa therapy, which is often used for the non-surgical treatment of loculated parapneumonic pleural effusions, may be associated with the development of haemothorax which may be severe with opacification of the treated hemithorax.
The use of intrapleural tPA therapy concurrently with antiplatelet therapy or prophylactic anticoagulation has not been shown to increase the risk of developing haemothorax to date, but the issues deserve further study.
Daily assessment of the patient’s clinical status, laboratory results, chest tube drainage and follow-up chest radiography based on the clinical picture are essential to monitor the clinical status of patients with loculated parapneumonic pleural effusions. This approach will allow the rapid identification of complications of intrapleural fibrinolytic therapy.
Footnotes
Contributors WHC planned collected data and prepared the initial manuscript. WHC and BKS finalised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.