Article Text

Statistics from Altmetric.com
Description
A 4-month-old girl visited our hospital’s emergency room reporting fever and coughing. She had been conservatively followed for prenatally diagnosed tricuspid atresia, complicated with a supernumerary rib and a radial defect after she was born at 38 weeks’ gestation with a birth weight of 2662 g. She had been coughing and vomiting especially during oral feeding since birth. Although the upper gastrointestinal series soon after birth revealed mild gastric volvulus, which was observed conservatively, she had been on duodenal tube feeding at home with persisted abdominal distension and poor growth.
She was admitted to the paediatric intensive care unit (PICU) and was intubated because of respiratory distress and anoxic spell. Aspiration pneumonia was first suspected because her sputum samples revealed various indigenous bacteria in the oral cavity, and she was commenced on antibiotics. Although mechanical ventilation with muscle relaxant started, gaseous intestinal distention persisted. Considering the above-mentioned anomalies as VACTERL association, we suspected H-type tracheo-oesophageal fistula (H-TEF). After her respiratory condition improved, we performed bronchoscopy (video 1), contrast-enhanced CT (figure 1) and the second upper gastrointestinal series (figure 2), which detected H-TEF. On day 12, the surgery was performed successfully, when the fistula was doubly ligated and transected with the cervical approach and left PICU on day 33.

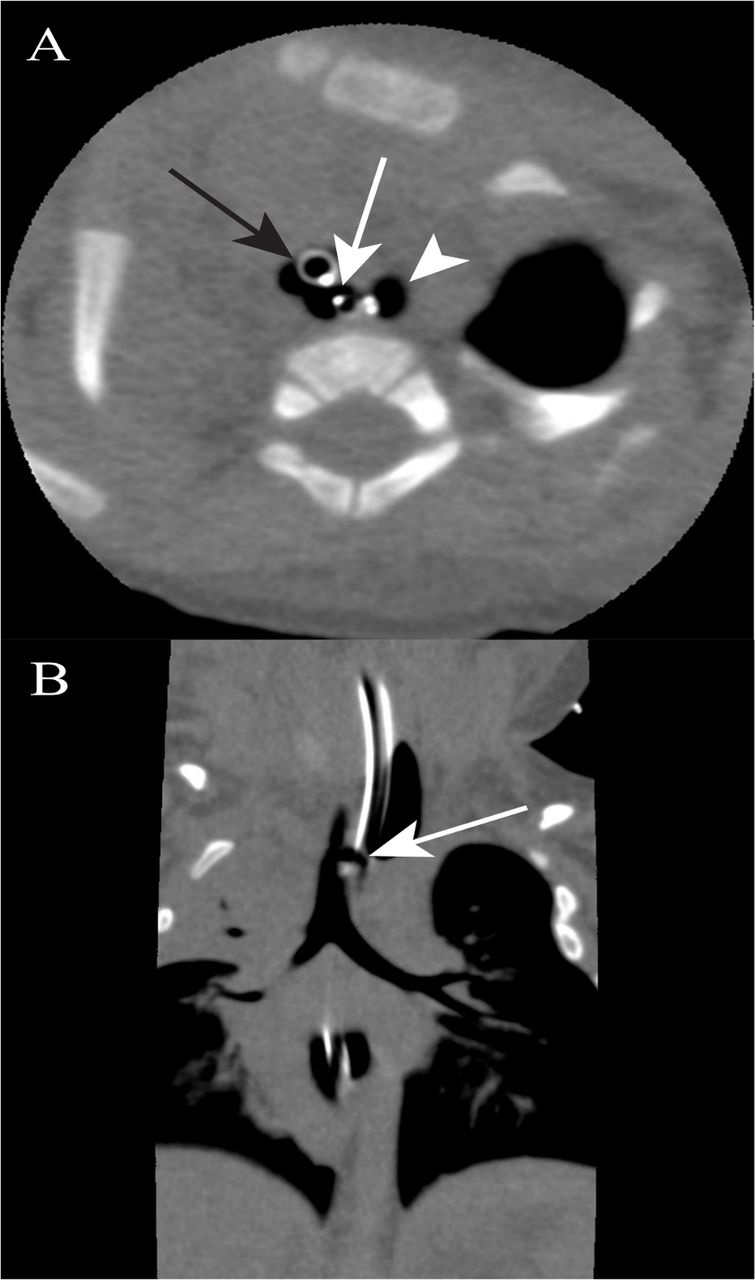
(A) Axial chest CT scan demonstrating trachea (black arrow), oesophagus (arrow head) and tracheo-oesophageal fistula (white arrow). (B) Coronal chest CT scan demonstrating tracheo-oesophageal fistula (arrow).

{kind=link}
{kind=link}
Oesophagography revealed trachea (black arrow), oesophagus (arrow head) and tracheo-oesophageal fistula at the T2 level (white arrow).
H-TEF accounts for approximately 5% of all tracheo-oesophageal malformations with an estimated incidence of about 1 per 100 000 live birth.1 The diagnosis can be delayed because the presentation is non-specific. Al-Salem and colleagues reported that clinical presentations with H-TEF are choking and coughing during an oral feed (52.2 %), recurrent chest infection (69.6 %) and cyanosis (43.5 %), and only one patient presented with abdominal distention.2 Several patients are diagnosed in late childhood and/or adulthood.3 4
The delayed diagnosis of H-TEF in our case may be explained as follows: coughing during oral feeding must have been caused by H-TEF, but the tube feeding improved the coughing, masking the typical symptoms of TEF. Cyanosis may have worsened during the oral feeding, but seemed to be overlooked, possibly because she was always cyanotic due to tricuspid atresia. Unexplainable abdominal distention after starting mechanical ventilation and the underlying anomalies provided a clue to H-TEF as part of the VACTERL association.
Although an oesophagogram is less invasive, a single examination can confirm the diagnosis in about 48 %.4 In our case, the first upper gastrointestinal series could not detect TEF soon after birth, partly because the examiner did not suspect H-TEF. Other diagnostic examinations include esophagoscopy, bronchoscopy and contrast-enhanced CT. Dai et al supposed that H-TEF was difficult to diagnose with a single examination, therefore, combined several examinations clarify the diagnosis.5 In our case, bronchoscopy was first selected as a diagnostic tool because she had already been ventilated, which clearly visualised H-TEF and prompted us to add CT and oesophagogram for the surgical team to plan the operative approach.
In summary, H-TEF is rare and the diagnosis is difficult due to non-specific symptoms, which might be masked by tube enteral feeding and/or underlying cyanotic heart disease. H-TEF should be considered for children with an intractable cough during an oral feed. A combination of several examinations is probably useful to diagnose with H-TEF and plan the approach for the surgery.
Learning points
A duodenal feeding tube and/or underlying cyanotic heart disease may mask the presentation of H-type tracheo-oesophageal fistula (H-TEF).
H-TEF should be considered for children with an intractable cough during oral feeding, particularly in patients with the VACTERL association.
Combination of several examinations is probably useful to diagnose with H-TEF and plan the approach for the surgery.
Footnotes
Contributors KY: made substantial contributions to the study’s conception and design, and acquisition, analysis, and interpretation of data. MW, HT, and MH: were involved in drafting or revising the manuscript critically for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.