Article Text

Abstract
We report two cases of anaplastic thyroid cancer (ATC) which had a very good response to a treatment with lenvatinib at 14 mg. A 73-year-old man with ATC stage IVB was operated on, undergoing a near-total thyroidectomy, and the pathological remnant tissue showed a quick and partial response to treatment with the drug. The patient had a single metastasis in the brain after 9 months, but then died due to bronchopneumonia after undergoing a neurosurgical intervention for the complete removal of the lesion. A 74-year-old woman with ATC stage IV was operated on, undergoing a near-total thyroidectomy after a neoadjuvant treatment with the drug, that was continued after surgical treatment. She had a partial remission of the local disease and of distant metastasis, which lasted for 14 months. She then died 4 months later due to cancer progression. Lenvatinib at 14 mg appears to be effective, fast and well tolerated.
- thyroid disease
- endocrine cancer
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Anaplastic thyroid cancer (ATC) is rare, but is one of the most aggressive cancers in humans. The standard treatment is surgical intervention, when possible, plus chemotherapy and accelerated hyper-fractionated external beam radiotherapy (EBR), usually in combination. 1 2 Despite this aggressive approach, prognosis is severe, and most of these cancers are metastatic at the initial diagnosis. Recently, targeted multi-tyrosine kinase (MTK) inhibitors have appeared to represent a further possibility for treatment to offer to these patients, and one of these, lenvatinib, has been approved in Japan for ATC (3–8). However, progression free survival (PFS) and overall survival (OS) in these patients, although dependent on stage, are still usually poor as regards any type of treatment, and, in fact, prognosis has not changed much over the last few years. We report an unusually long PFS and OS in two consecutive patients treated with a low-intermediate dose (14 mg) of lenvatinib, and speculate about possible explanations.
Case presentation
Case 1
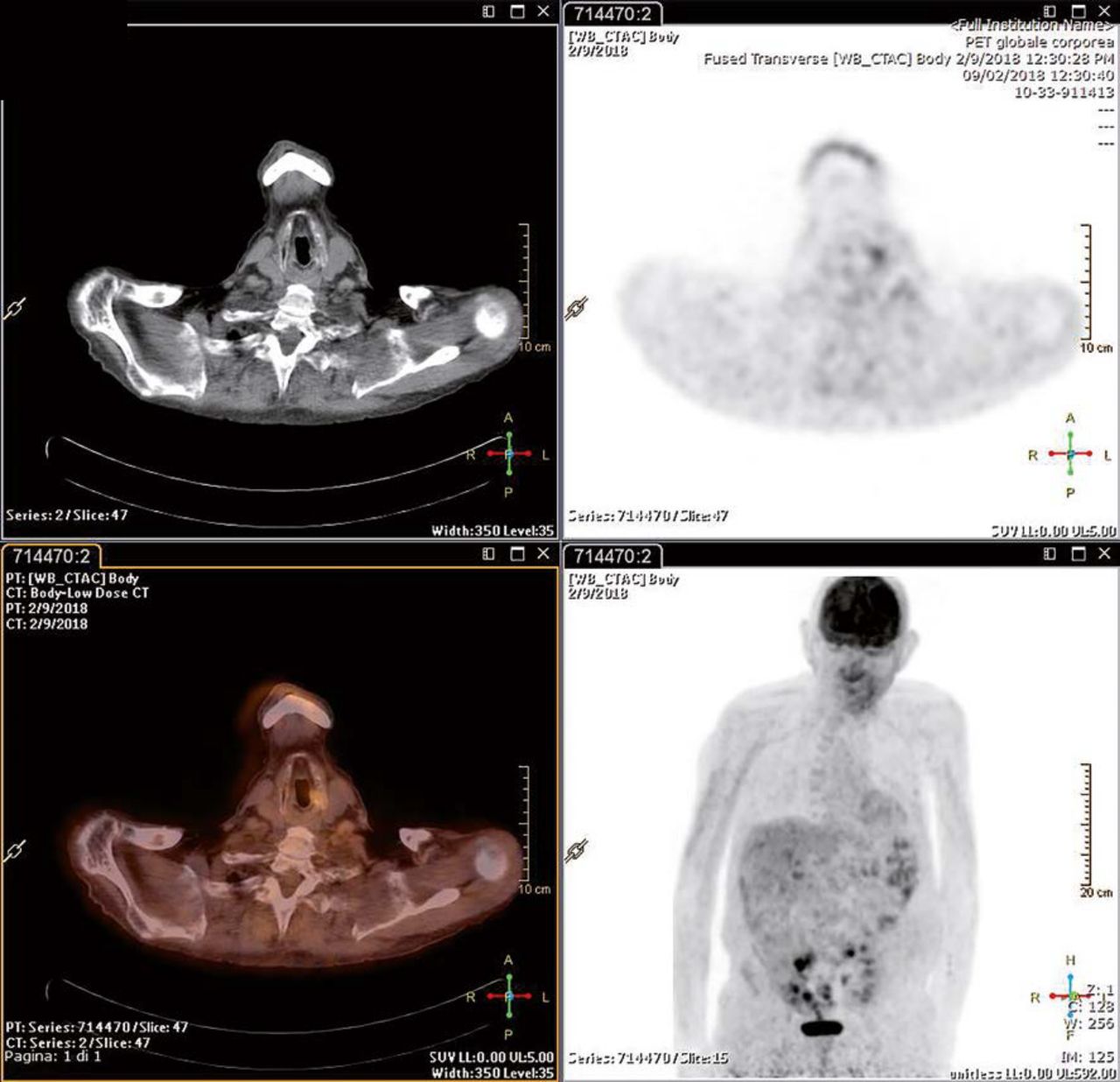
A 74-year-old male patient had already undergone a kidney transplant, and he was under treatment with everolimus and ciclosporin. He was in follow-up for inflammatory myofibroblastic tumour of the lung already treated by surgical intervention. During the follow-up, a CT/positron emission tomography (PET) showed a thyroid mass with high uptake (standardised uptake value/SUV 20.1) (figure 1). An ultrasonography confirmed a mass of 7.0 in maximum size in the left lobe and isthmus with a suspected lymph node metastases. A fine needle aspiration (FNA) was suspicious for ATC. The patient, after stoppage of everolimus, was sent for surgical treatment, and it was possible to perform a near-total thyroidectomy, leaving some paratracheal pathological tissue. The histology was: ATC with maximum size 7.5 cm involving the left and right lobe with spindle growth pattern, infiltrating perithyroidal muscles and oesophagus (immunophenotypic investigation showed CKAM 5.2 positive, TTF1 and thyroglobulin negative), one lymph node with metastasis, pT4aN1bMx stage IVB TNM 2017 8th edition. Considering the general clinical context, after obtaining written consent for an off-label treatment, we decided to treat the patient with lenvatinib, and we chose as first line a medium-low dosage of 14 mg, which was initiated 7 days after the surgical intervention.

Whole body (18F)fluorodeoxyglucose positron emission tomography/CT before surgical intervention.
Molecular analysis of tumour pathological tissue was performed, and the data are reported in table 1.
Molecular analysis was performed on DNA from formalin-fixed paraffin-embedded tissue
Outcome and follow-up
After 3 weeks we performed a first (18-fluorodeoxyglucose (18-FDG)) PET/CT, which showed a pathological tissue remnant with SUV 5.1 (figure 2). Ultrasonography showed only a small paratracheal pathological remnant tissue. Another (18FDG) CT/PET performed at 4 and 8 months, showed only minimal remnant tissue in the neck with a further reduced uptake, SUV 3.1 (figure 3). The patient was in good health, with an Eastern Cooperative Oncology Group (ECOG) score of 1–2. After 9 months, the patient had seizures, and an MRI showed a mass of 2 cm (a previous MRI 2 months before had been negative). The patient underwent neurosurgical intervention with complete removal of the lesion, but he passed away after 10 days due to bronchopneumonia.

Whole body (18F)fluorodeoxyglucose positron emission tomography/CT after 3 weeks of treatment.
Whole body (18F)fluorodeoxyglucose positron emission tomography/CT after 8 months of treatment.
Case presentation
Case 2
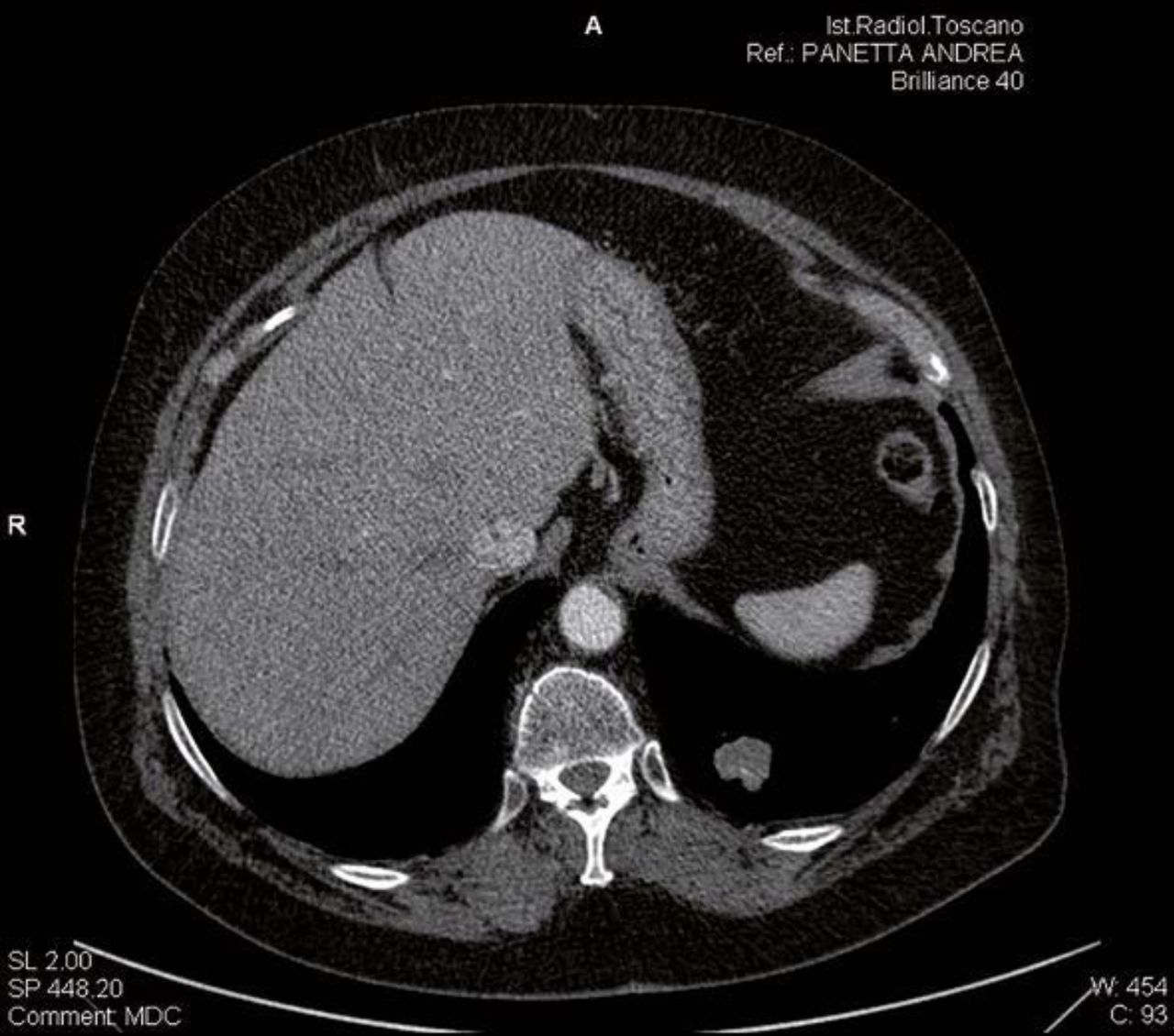
A 73-year-old female patient presenting with a rapidly growing goitre. At that moment the patient was in good health, and her ECOG score was 0. FNA was suspicious for ATC, and the patient underwent Computerized Tomography) (CT) total body, which showed a mass in the neck which extended into the mediastinum and apex of the lung, as well as lung metastases (figures 4 and 5). During staging, the patient showed not only a visible increase of the mass in the neck, but also a worsening of well-being, with diffuse pain in the chest and rapid deterioration of her clinical status. The patient was referred for surgical treatment, but she refused it, knowing the poor prognosis of the disease and the possibility that the intervention could be only a debulking with positioning of a tracheal cannula.

Chest CT scan at first staging.

CT scan: prevalent lung metastasis at the first staging.
Molecular analysis of tumour pathological tissue was performed, and the data are reported in table 1.
Outcome and follow-up
We decided, after written consent, for the off-label use of lenvatinib, and we started the drug at 14 mg/day. At that moment ECOG was 1/2. The patient did not show side effects, and experienced some improvement in quality of life in the first week regarding pain in the chest. A CT scan performed after 3 weeks showed a decrease in the mediastinal mass (figure 6). At this point we exerted great effort to convince the patient to submit to surgical treatment, and she agreed. The histology showed an ATC with a maximum size of 7 cm infiltrating perithyroid muscle TTF1, thyroglobulin, CD30 negative; CKCAM 5.2 positive, pT3bNxcM1 TNM 2017 8th edition stage IVC. During the following months, imaging showed a progressive remission of the disease up to almost complete remission (figures 7 and 8). After 14 months she experienced recurrence with unilateral palsy, and a CT scan showed progressive disease in the mediastinum and chest. Subsequently, the patient developed bilateral recurrent palsy, and underwent a tracheostomy. Exitus occurred after 4 months.

Chest CT scan after 3 weeks of treatment.

Chest CT scan after 12 months of treatment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chest CT scan with contrast medium: prevalent metastasis after 12 months of treatment.
Discussion
ATC is one of the most malignant solid tumours in humans. The prognosis is usually so poor that there is not any real guideline regarding treatment, although surgical intervention is usually considered the first line of treatment.1 2 It can have a debulking aim, or, rarely, offer a possibility of radicality in less advanced cases, and sometimes surgical treatment can follow an attempt of neoadjuvant medical treatment. The type of medical treatment, alone or combined with EBR, still represents a matter for discussion, and among medical treatments, some MTK inhibitors, already approved for iodine refractory differentiated thyroid cancer, have garnered interest. Among these, lenvatinib is known to be directed against FGR 1, 2, 3, 4; VEGFR 1, 2, 3; PDGFRb; RET and c-Kit, and it has been successfully employed in iodine refractory thyroid cancer.3 Lenvatinib has been approved also for treatment of ATC, in Japan in 2015, and there are now several reports regarding this drug.4–9 However, in advanced stages IVB and IVC, as in our cases, the PFS and OS are usually poor. The various published papers have shown a median of PFS and OS ranging, respectively, from 4.0 to 4.2,5 and 7.4 to 10.6 months.5 6 The best results appear to be those of a phase II study.5 6 However, in this study a partial response was seen in only 24% of cases, and only 4 patients out of 17 were able to complete the study, either because they did not show a response, or because they developed severe side effects to the treatment at the initial dose of 24 mg. In this last study, the patients enrolled had as a criterion of inclusion that they were expected to survive at least 8 weeks or more after the first dose of lenvatinib, so we must also suppose that their clinical condition was not so bad. The stage for all patients was between IVA and IVC, but it was not reported which cases were able to finish the study and showed the best results.
Our cases offer interesting points for speculation. In our first case, we had a PFS of 8 months, and the recurrence of disease was in the brain. There are no data regarding the crossing of lenvatinib through the blood–brain barrier, but as regards other MTK inhibitors we can suppose a reduced transfer in the brain, and therefore a reduced concentration and activity at this level.10–13 On the other hand, no locoregional recurrences in other sites of the body were present. Rather, lenvatinib appeared to exert very good locoregional control, inasmuch as CT/PET showed a very remarkable reduction of FDG uptake in the neck. The overall survival was 10.2 months, but it could have been much longer if the patient had not passed away because of bronchopneumonia, due likely to the immunosuppressive treatment, since the neurosurgical intervention removed completely the metastasis. The second case appears even more surprising, considering the stage and the general clinical condition. We had a PFS of 14 months, with an OS of 18 months, and a partial remission which came very near to a complete remission. Both patients tolerated quite well the starting dose of 14 mg, considering the fact that the side effects were related to the dose and to the serum levels.14–16
An initial speculation could be that in the complex mechanism of the regulation of the various MTK cascades, there could exist a specific, most effective dose, beyond which a hook effect occurs, and the efficacy may decrease. Although data in vitro show that the effects on ATC cells of lenvatinib are dose dependent,17 18 no study, in point of fact, reports if there might exist something like this hook effect for an increasing dose of the drug. If we analyse all the cases reported in the literature, we find only two cases comparable both for advanced stage and for PFS (9.0 and 27.9 months)3; also in these series some patients were treated with 14 mg for a progressive reduction of the drug, but, unfortunately, in that paper it is not specified which dose these two cases were treated with.
We could also speculate that in our cases we enjoyed such a good response because the dose of lenvatinib was not very high, and was hence well tolerated by the patients, who could continue without important side effects, being that side effects were related to the oral dose.14–16 However, the response was not only long-lasting, but also fast, showing powerful activity of the 14 mg of lenvatinib. Regarding the first hypothesis, that there is the possibility that this intermediate dose might exert some special activity on ATC, studies in vitro will help to show the dose/activity profile of the drug. As already stated, some studies exist showing a dose-dependent activity.17 18 However, higher concentrations will have to be studied, even though we have to keep in mind that studies in vitro on ATC cells cannot represent the reality in vivo, since lenvatinib exerts a fundamental action also on the vessels by Vascular Endothelial Growth Factor .
Regarding molecular analysis, our data do not appear to show any special predictive mutation for a better response.
In conclusion, in our two consecutive cases treated by lenvatinib, we enjoyed a very good response using 14 mg. Further studies in vitro and clinical trials should be encouraged to test lenvatinib in ATC using lower doses than the standard 24 mg dose. From a practical point of view, we could suggest trying to use this particular dose (14 mg) as a starting dose in such critical patients with ATC, since the drug is effective, the action is fast, and side effects are seen to be less frequent and more manageable.
Learning points
Diagnosis of anaplastic thyroid cancer (ATC) is usually histological. However, in special cases a cytology examination by an expert pathologist can be sufficient (case 2).
Lenvatinib at low-medium dosage (14 mg in our cases) has been demonstrated to be highly effective and quick in controlling the disease. Two possible explanations can be speculated on: simply that this lower dose can allow a better treatment of patients because of the absence of important side effects in such critical patients, or that an especially powerful activity of an intermediate dosage is exerted on the complex balance of multi-tyrosine kinase cascade in ATC.
Research in vitro and clinical trials could help to elucidate the hypothesis that a lower dosage could be more effective than a full standard dose in this cancer.
Lenvatinib can have a neoadjuvant role (case 2).
References
Footnotes
Contributors DB: writing of the manuscript. PL: references and editing figures. PV: cytology. LT: histology and molecular biology.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.