Article Text

Abstract
Pheochromocytomas are uncommon tumours that originate in chromaffin cells. They are a representation of 0.1%–1% of all cases of secondary hypertension. Most pheochromocytomas are unilateral and benign, featuring catecholamine production, as well as the production of other neuropeptides. Pheochromocytomas are mostly located in the adrenal gland; the frequency of occurrence is highest between 30 and 50 years of age; however, up to 25% of cases may be linked to multiple endocrine neoplasia type 2, Von-Hippel-Landau disease and type 1 neurofibromatosis in the young.
We present a case of ruptured left adrenal pheochromocytoma with an atypical presentation. A 30-year-old male patient presented with severe left flank pain and hypertension. The CT scan of the abdomen showed bleeding from the left adrenal mass, where resuscitation and angioembolisation were done. Embolisation of the inferior and superior arteries was done, but the middle failed. The patient experienced a significant drop in haemoglobin and a haemorrhagic shock post angioembolisation, which called for emergency laparotomy. The patient is currently doing well with an uneventful postoperative course.
- emergency medicine
- resuscitation
- adrenal disorders
- endocrine cancer
- radiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Pheochromocytomas are rare tumours that affect the sympathetic nervous system. They originate from the adrenal medulla chromaffin cells. Most pheochromocytomas are unilateral, at least in 90% of cases. The prevalence of bilateral disease is higher in the paediatric population and associated with genetic syndromes. Tumours are more common on the right adrenal medulla, with a higher preponderance to trigger paroxysmal hypertension. Conversely, left-sided tumours cause persistent hypertension. According to recent studies, these tumours are seen in at least 2–8 cases per million per year.1 It is also associated with less than 0.1% of hypertension cases, although 90% of patients with pheochromocytoma have hypertension.2 Pheochromocytoma presents with symptoms such as diaphoresis, headaches and palpitations. Elective surgery is considered as the gold-standard treatment. Of course, this comes post-antihypertensive therapy course, which usually lasts a week or two.
The term pheochromocytoma multiple system crises (PMC) was coined.3 PMC is a rare and fatal condition that presents with symptoms such as encephalopathy, instability and collapse of haemodynamics, multiorgan failure and hyperthermia. It is important to note that there is no clear-cut association between PMC and hypertensive crisis. It is common to find incidences of labile blood pressure in PMC patients. The blood pressure ranges from hypotension to extreme cases of hypertension (60–250 mm Hg). However, its treatment is controversial as clinicians are yet to reach a consensus regarding the timing of adrenalectomy in the specific setting of the pheochromocytoma crisis.
The medical management of pheochromocytoma should come prior to surgical resection.4 Traditionally, PMC treatment consists of immediate medical stabilisation in the emergency setting and then urgent or emergent adrenalectomy. Stabilisation of the patient in the form of securing the airway, assisting breathing, supporting the circulation and pain management is the primary goal of managing patients with PMC in the emergency department. Timely diagnosis and management of the pheochromocytoma patients presented with life-threatening conditions such as haemorrhage, acute pulmonary oedema, myocardial infarction, acute renal failure and multiorgan failure are the mainstay of management in the emergency, and critical care setting, including blood pressure control with an alpha blockade, fluid infusion therapy and transcatheter arterial embolisation (TAE), are the alternatives for controlling the haemorrhage.5
Treatment options for PMC include emergent adrenalectomy, urgent adrenalectomy and elective adrenalectomy.6
Case presentation
A 30-year-old Tunisian man has presented to Hamad General Hospital, a tertiary hospital in the state of Qatar, with severe left flank pain associated with headache. The patient was sweating, anxious, and in excruciating pain. He reported diffuse left-sided chest pain and shortness of breath. He denies fever, vomiting, diarrhoea, trauma, haematuria or any urinary manifestation. He had an episode of chest pain 1 month ago for which he was treated in another hospital as non-ST segment elevation myocardial infarction. The patient was married without children and a nonsmoker. The patient gave a history of high blood pressure a few months ago when his general practitioner started him on amlodipine 5 mg, which he used for a week and stopped with no follow-up. The patient had no known allergies.
The physical examination yielding that his blood pressure was 162/102 mm Hg, his monitored heart rate was 116 bpm, his respiratory rate was 21 per minute, his oxygen saturation was 98%, and he was afebrile.
He was fully conscious and had no neurological deficit. Chest and heart examination were unremarkable. The abdomen was distended with tenderness on the left side. His extremities examination showed equal bilateral peripheral pulses with no signs of deep vein thrombosis.
Bedside point-of-care ultrasound (POCUS) showed no hydronephrosis bilaterally, no free fluids, a normal diameter of the aorta. The heart has normal contractility, no right-sided strain and had no pericardial effusion.
Investigations
His complete blood count (CBC) showed leucocytosis and mild anaemia (haemoglobin 12.4 g/L and haematocrit 37.5 %). He had mild renal impairment as his creatinine was 170 µmol/L. His remaining blood investigations, including electrolytes and liver function, were within normal limits (table 1). Cardiac markers were within the normal range. Urine analysis was normal. His ECG did not show acute ischaemic changes. The chest X-ray was normal, with no pneumothorax or pneumonia.
Baseline blood investigations
CT of the abdomen and urinary tract (figure 1) showed a large soft tissue like lesion at the left adrenal region with hyperdensities. For the best illustration of the mass, the radiologist asked for a CT angiography (figure 2), which showed posteromedial active extravasation of contrast seen on the arterial phase fade mostly at the delay phase. This lesion measured 9.7×12.3 x 12.6 cm in transverse, anteroposterior and craniocaudal dimensions. The lesion was pushing the left kidney downward and laterally with severe surrounding fat stranding and perinephric fluid. No significant hydronephrosis was noted in both kidneys with normal kidneys enhancement bilaterally. No stones were noted along the kidney and urinary bladder axis.
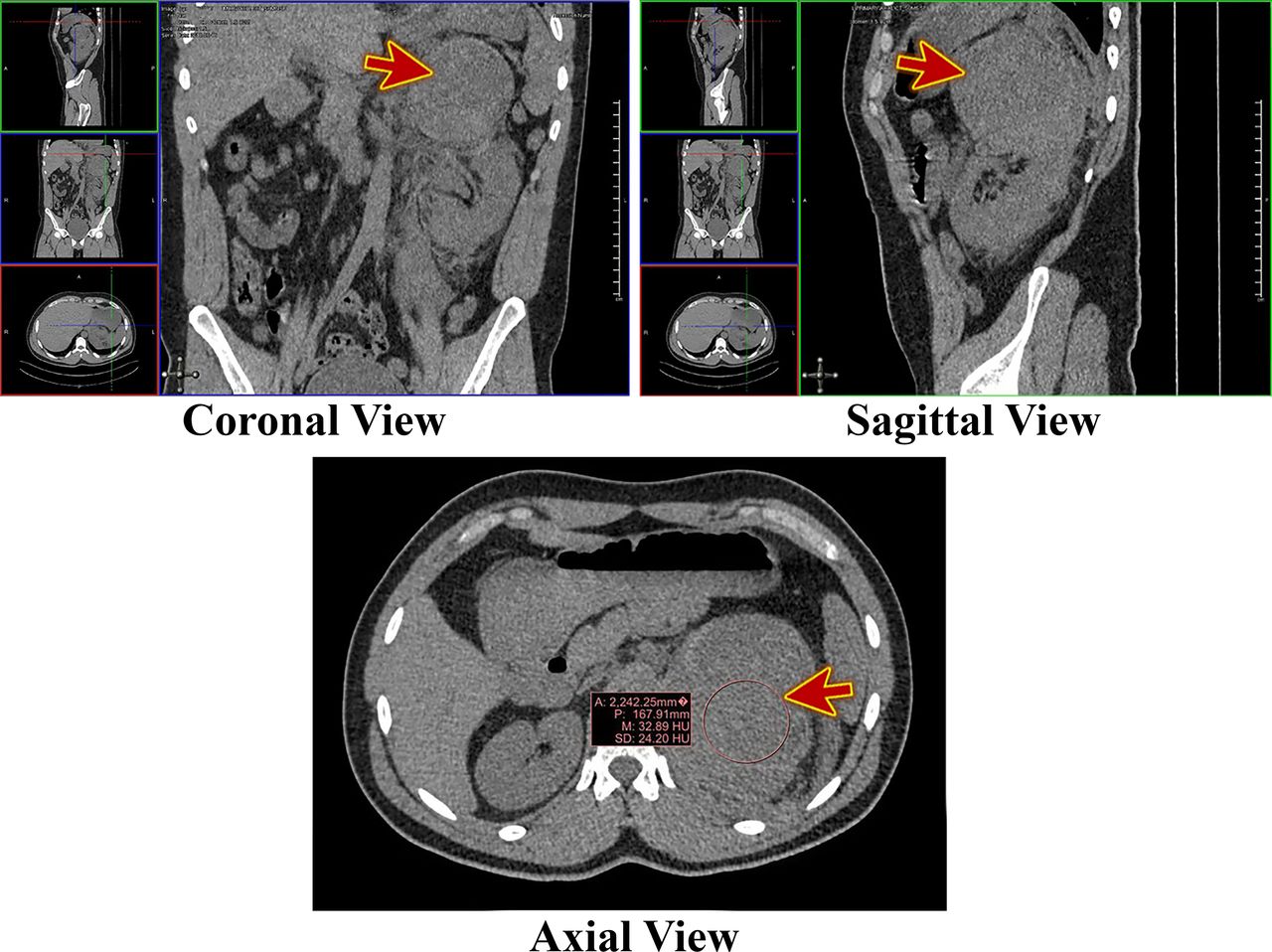
CT of the abdomen and urinary tract showed a large soft tissue like lesion at the left adrenal region with hyperdensities within (red arrow), pushing the left kidney downward and laterally with severe surrounding fat stranding and perinephric fluid.

CT abdominal angiography showed posteromedial active extravasation of contrast seen on the arterial phase (red arrow), venous phase (blue arrow), and fade mostly at the delay phase (green arrow).
Differential diagnosis
The patient presented to the emergency department with a picture of acute renal colic with a hypertensive emergency in the form of high blood pressure, chest pain and shortness of breath. His ECG did not show ischaemia. Bedside POCUS did not show hydronephrosis bilaterally and normal diameter aorta. Cardiac markers were within the normal range. The contrast-enhanced CT abdomen concluded that there was a large left adrenal region haematoma with active bleeding.
Treatment
The patient had a CT of the abdomen and urinary tract showed a significant soft tissue like lesion at the left adrenal region. The radiologist preferred to do another CT angiogram while the patient was on the table, which showed bleeding from the left adrenal mass. The patient’s clinical condition was monitored by serial measurement of the vital signs, CBC, arterial blood gases, and urine output. The patient received intravenous phentolamine (alpha-blocker) to control his blood pressure. During this period, the patient was haemodynamically stable, and there was no drop of haemoglobin (12.4 g/dL) and haematocrit (37.5 %). Left adrenal artery angioembolisation after 12 hours from the patient’s presentation on a life-saving basis was done (figure 3). No immediate complications were encountered, and there was no extravasation postembolisation.

Transarterial selective left adrenal artery embolisation; selective catheterisation of the left superior adrenal artery (A), selective catheterisation of the left inferior adrenal artery (B), embolisation with a tiny amount of 350–500 particles (C).
Postangiography, the patient was admitted into the surgical intensive care unit (ICU), where he continued to have tachycardia with high blood pressure; oral prazosin 1 mg (alpha-blocker) was commenced, and the blood pressure was monitored every 1 hour through an arterial line measurement (table 2).
Serial blood pressure measurement
Serial CBC showed a drop in haemoglobin to (7.1 g/L) and haematocrit (23.3 %), and the patient’s condition deteriorated, so three units of packed red cell count were transfused, then he was taken for emergency laparotomy. Later, the patient did well with an uneventful postoperative course.
Outcome and follow-up
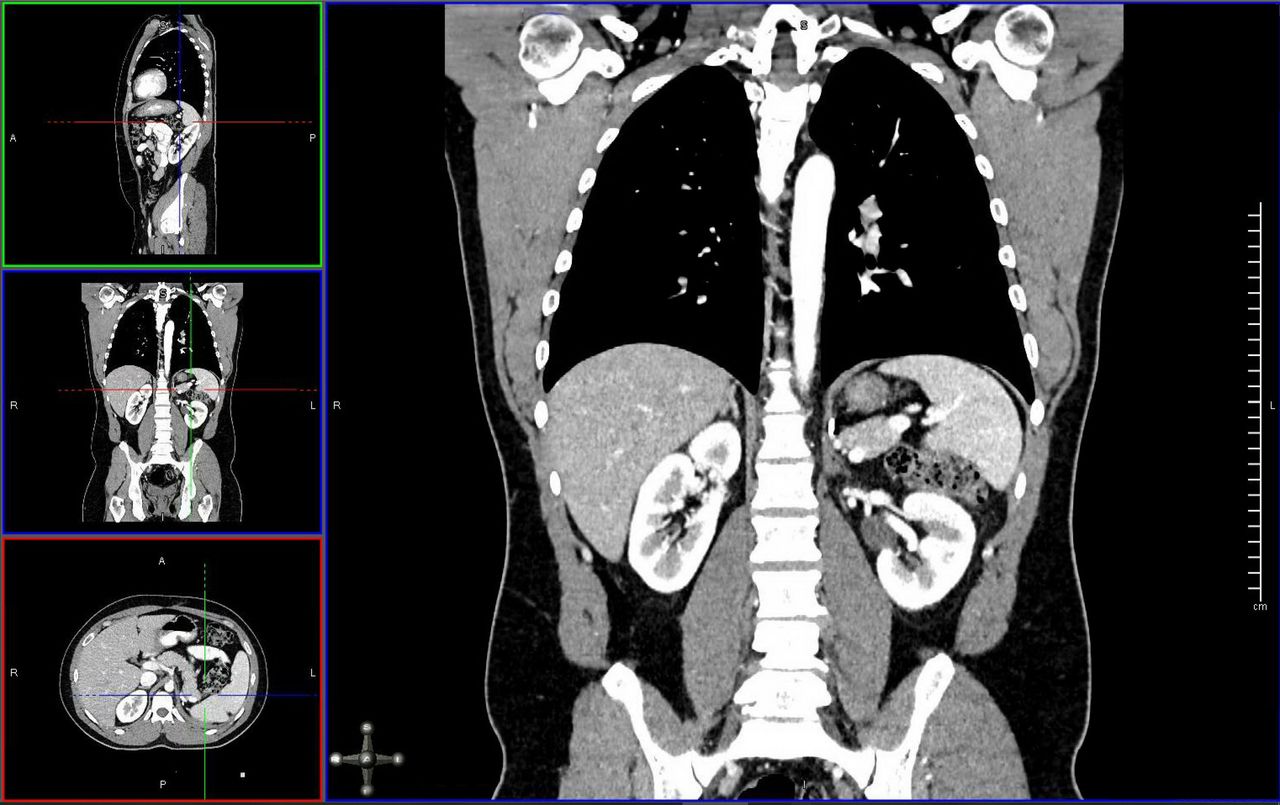
The patient had a smooth postoperative course, and his blood pressure improved on alpha-blocker medications. He was discharged and following with the endocrine and oncology team in outpatient clinics. The surgical pathology report showed a pheochromocytoma with mitotic figures greater than 4/10 per high-power fields (2), high cellularity (2), large nests or diffuse growth (2) and focal or confluent tumour necrosis (2). So, the total Pheochromocytoma of the Adrenal Gland Scaled Score was 8 over 20 (Scores exceeding four predicts an aggressive potential and aggressive behaviour). He underwent a regular follow-up CT scans and a regular follow-up with catecholamines in urine yearly, and he did not show recurrence until now (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Follow-up CT abdomen with contrast showed no recurrence of the mass.
During the outpatient follow-up visits, the patient’s blood pressure was controlled without medications, and he did not develop any pain. Whole-body fluorodeoxyglucose-positron emission tomography done on 2 September 2020, showed that there is no evidence of 6-[18F]fluor-l-3,4-dihydroxyphenylalanine avid lesion to suggest metastatic or recurrent disease.
Discussion
Rupturing of adrenal pheochromocytoma is very rare. In the most cases, it can be lethal. The first report of this condition was doneby Cahill. Since then, a total of 50 cases (38 cases of ruptured pheochromocytoma, and 12 cases of haemorrhagic) have been reported between the 1950s and 2000s globally. It has a 34% mortality rate globally.7–10 A 2008 study described a case of PMC after induction of general anaesthesia in the context of elective adrenalectomy for an established case of pheochromocytoma, despite the preoperative blockade.11 The clinicians aborted surgical resection, and the patient was moved to a facility and confined to the ICU for 6 days where his medical condition was stabilised, after which he underwent urgent adrenalectomy. The multisystem organ failure resolved, and the patient was discharged after a month.
A 2010 study reported a case of PMC that presented with encephalopathy and acute respiratory failure. In this case, surgical resection was carried out 11 days after a patient’s admission due to progressive deterioration of the patient’s medical condition.12 There was a significant improvement in the patient’s condition after the operation and resolution of the multisystem organ failure. However, the patient still had to undergo long-term haemodialysis due to chronic renal failure.
Another study reports the case of a patient who struggled with acute heart failure with cardiogenic shock refractory to inotropic pharmacotherapy. There was a need for the insertion of an intra-aortic balloon pump. The clinicians also considered extracorporeal membrane oxygenation. However, the physicians involved who took charge of the treatment chosen to perform emergent adrenalectomy. This resulted in a great improvement in the patient’s respiratory and haemodynamic status after surgery.13
Preoperative mortality is mostly caused by hypovolaemia due to haemorrhage, heart failure due to catecholamine cardiomyopathy, and respiratory disorder due to pulmonary oedema.10 The precise cause and mechanism of pheochromocytoma are not fully understood. Rapid tumour development and intratumoural haemorrhage may trigger an increase in capsule pressure, thus resulting in rupture. After rupturing, a huge amount of catecholamine is released into the general circulation, triggering severe headache, hypertensive crisis, nausea, vomiting, abdominal pain, ileus, sweating, pale skin and serum creatinine elevation.14 Pheochromocytoma before the operation is challenging. A report by Kobayashi et al shows that there is only a 30.2% correct preoperative diagnosis rate. The difficulty in making a diagnosis may arise from the rarity of the incidence. Also, the determination of catecholamine levels in either urine or serum is not possible under emergency conditions.7
Surgical resection is the treatment of choice, and it may be done either through elective or emergency operation. The major prognostic factor is effective in controlling blood pressure with an α-adrenergic blockade and fluid replacement preoperatively. According to a literature review, emergency surgery carried out without proper control of blood pressure and wrong preoperative diagnosis has a strong link with poor prognosis.10 A study showed that of the two cases recorded in Korea where an emergency operation was done without control of blood pressure, one case died due to pulmonary oedema and heart failure.11 12 Patients who do elective surgery post medical therapy experience no mortality.10 Alpha-blockers like phenoxybenzamine are used for preoperative management of hypertensive crisis as they have the capability of blocking adrenoreceptors. Propranolol helps to resolve cardiac arrhythmia.15 Angiographic intervention is helpful for active bleeding and rupture, as seen in our patient. A study by Habib et al16 highlighted three ruptured pheochromocytoma cases with rupture and bleeding treated successfully by elective resection after blood pressure control via TAE. The glands are supplied by the superior, the middle and the inferior suprarenal arteries. These arteries originate from the inferior phrenic artery, the abdominal aorta, and the inferior suprarenal arteries, respectively.17 Alpha-adrenergic blocker can also be used to achieve blood pressure control, the same with fluid infusion therapy or after stabilisation by TAE.18 Postoperative TAE helps with haemostasis and is devoid of complications like hypovolemic shock.16 Pains in the abdominal region are associated with stimulation of the α-adrenergic receptors, intestinal vascular smooth muscle constriction, and ileocolic sphincter contraction. Catecholamines circulating at high levels will cause a decrease in intestinal motility and tone.19 The application of TAE enhances haemostasis and consolidates the haematoma.20
Patient’s perspective
I visited the hospital for seeking help for severe agonising left-sided body pain, and I thought that it was renal colic. I never imagined that there was a tumour. All the family and I are happy with the management I had at the hospital and would like to thank all the medical team for their compassionate care.
Learning points
Pheochromocytomas are rare-occurring tumours that secrete catecholamines. Rupturing of adrenal pheochromocytomas is an infrequent occurrence. It is a fatal condition due to the rapid and sudden changes that take place within the general circulation.
Ruptured pheochromocytoma can be presented by pain and hypertension, which preceding hypovolemic shock.
To date, the precise mechanism of pheochromocytoma is not known. However, high blood pressure caused by excess catecholamines’ release contributes to vasoconstriction in the tumours, leading to necrosis, high intracapsular pressure and haemorrhage. High pressure in the intracapsular region can tear off the capsule, leading to haemorrhage (retroperitoneal).
Close monitoring of the patient’s condition and serial complete blood count is the mainstay to detect early deterioration and ongoing bleeding.
In the ruptured pheochromocytoma, antihypertensive medications (alpha-blocker), resuscitation by transfusion of blood products, and haemostasis by transcatheter arterial embolisation are life-saving procedures until adrenalectomy carried out.
Acknowledgments
We want to thank Thirumoothy Samy Suresh Kumar for his valuable revision of the case.
References
Footnotes
Twitter @amamiro2000
Contributors AmE manuscript writing, images, review. MY: manuscript writing, clinical care. AhE: radiology images. KB: review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.