Article Text

Abstract
A 59-year-old Caucasian man infected with HIV, in remission from human herpes virus-8-positive extracavitary primary effusion lymphoma (EC-PEL), presented to a sexual health clinic with fever and rectal pain 10 weeks after a single episode of receptive anal sexual intercourse with another man. He was initially treated for a presumptive diagnosis of lymphogranuloma venereum proctitis, then for syphilis on positive serology. Rectosigmoidoscopy revealed a single ulcerated rectal mass; endoscopic biopsies confirmed the recurrence of EC-PEL. The patient received chemotherapy and went into remission. This is the first reported case of EC-PEL occurring synchronously with early syphilis, and specifically at the site of inoculation, which can be a major diagnostic challenge since both conditions may present with lymphadenopathy, mucosal involvement and constitutional symptoms. We reviewed the literature for similar cases and hypothesised that syphilis may have triggered the recurrence of this rare lymphoma.
- infection (gastroenterology)
- HIV / AIDS
- colon cancer
- syphilis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Primary effusion lymphoma (PEL) is a very aggressive rare subtype of large B cell lymphoma1 2 with a median survival of less than a year.3 4 This lymphoma usually occurs in individuals infected with HIV4 5 and among recipients of organ transplants.6–8 Human herpes virus-8 (HHV8)/Kaposi sarcoma-associated herpesvirus (KSHV) is an oncogenic virus involved in all cases of PEL, with 80% concomitant association with Epstein-Barr virus (EBV).9 Conversely, while HIV-negative patients with PEL from HHV8 endemic areas such as the Mediterranean are older, EBV infection occurs in only 50% of cases and is associated with more extracavitary involvement.10 11 PEL typically presents as a malignant effusion in the pleural, pericardial or peritoneal cavities.3 However, in 5% of cases,2 lymphomas otherwise indistinguishable from PEL presenting as solid tumour masses outside body cavities have been recognised by the WHO revised fourth edition as the extracavitary variant of PEL (EC-PEL).12 EC-PEL most commonly presents in the lymph nodes and skin3 13; however, cases of gastrointestinal involvement5 9 14–17 have been reported and their outcome seems to be better than the effusion variant.3
Syphilis, a sexually transmitted disease caused by the bacterium Treponema pallidum, is a source of substantial morbidity, complications and adverse outcomes.18 Syphilis is a major public health concern as the number and rates of reported cases are rising dramatically in Western Europe and the Americas,18 including Canada, where they have more than doubled since 2008 and have the highest increase in rates of all sexually transmitted disease.19 As syphilis is a great masquerade20 and may present as generalised lymphadenopathy and fever,20–22 diagnosis of a synchronous lymphoma represents a diagnostic challenge.
The case we present herein illustrates both the very rare occurrence of EC-PEL within the digestive tract and the diagnostic challenge posed by simultaneous early syphilis. To our knowledge, this is the first reported case of EC-PEL occurring synchronously with early syphilis specifically at the site of inoculation. This observation led us to raise the hypothesis that syphilis played a role in the recurrence of this rare lymphoma.
Case presentation
A 59-year-old Caucasian man with a long history of treated HIV infection presented to a sexually transmitted infection (STI) clinic in October 2019 with complaints of rectal pain and fever. He was initially diagnosed with HIV infection in 2010 with a low CD4 T cell count of 60×106/L and plasma HIV viral load of 151 000 copies/mL and was successfully treated with emtricitabine, tenofovir and raltegravir. He was later diagnosed with cutaneous Kaposi sarcoma (KS) with bilateral inguinal lymphadenopathy in 2012 and with HHV8-positive but EBV-negative EC-PEL with cutaneous involvement in 2014.2 He was treated with liposomal doxorubicin (LD) for his KS and with four cycles of R-CHOP (rituximab, cyclophosphamide, doxorubicin hydrochloride, oncovin and prednisone) for his lymphoma, as previously described.2 His CD4 T cell count remained below 100×106/L on the same antiretroviral therapy (ART), and although he had recurrences of his lymphoma (2015–2017) involving the skin and tonsils without lymphadenopathy he had been in remission since October 2017.
His rectal pain developed 3 weeks after a single episode of receptive anal sexual intercourse with another man, precisely on 29 June 2019. On 7 October 2019, he presented to an STI clinic in Montreal with worsening rectal pain, tenesmus, mucoid discharge, constipation alternating with diarrhoea, and fever (38.4°C). He also complained of severe constitutional symptoms, including drenching night sweats, weight loss (about 9 kilogram) and extreme fatigue. He denied any bright red blood per rectum, melaena or vomiting. Physical examination of his palms, soles, torso, penis, anus, mouth, spleen and lymph nodes was unremarkable, and no lesion or ulcer was identified.
Investigations
On 7 October 2019, the patient underwent serological testing for syphilis, and samples from the throat, anus and penis were collected for sexual screening, including testing for Chlamydia trachomatis and Neisseria gonorrhoeae. Based on clinical presentation, he was treated with doxycycline for suspicion of lymphogranuloma venereum (LGV) proctitis. However, the nucleic acid amplification test (NAAT) for chlamydia and gonorrhoea was negative, excluding LGV proctitis. Testing for syphilis showed a high rapid plasma reagin (RPR) titre of 1:128, consistent with early syphilitic infection. Treatment with penicillin was initiated, followed by a decline in fever, night sweats and relief in his constipation, accompanied by a rapid decline in the levels of inflammatory markers such as β2 microglobulin, C reactive protein (CRP) and D-dimer (0.75 µg/mL) (table 1). Furthermore, following penicillin treatment, the RPR titre declined from 1:128 to 1:8 and further to 1:2 on 19 December 2019 and 10 January 2020, respectively (table 1) However, T. pallidum was not identified on biopsies by immunohistochemistry performed 10 days after treatment for LGV and syphilis.
Summary of the patient’s serological test results before and after relapse of EC-PEL
The patient underwent rectosigmoidoscopy on 17 October 2019, which revealed a 5 cm rectal mass, of which multiple biopsies were taken. The patient was also referred to his haematologist at the McGill University Health Centre where he had been followed and treated for his lymphoma. Whole-body positron emission topography/computed topography (PET/CT) scan revealed intense 18-fluorodeoxyglucose (FDG) activity in the rectum and hypermetabolic activity in the left external iliac, porta hepatis and internal mammary lymph nodes, most consistent with a lymphoproliferative process.
Histopathological analysis of the endoscopic biopsies showed fragments of the tissue consistent with ulceration and infiltration by large atypical lymphoid cells (figure 1). Immunohistochemistry revealed that the neoplastic cells were positive for HHV8, Epithelial Membrane Antigen (EMA) and B-cell lymphoma 2 (BCL2) and negative for CD45, CD3, CD20, CD79a, PAX5, BCL6, CD30, CD15 and CD138. Kappa and lambda light chains were negative by in situ hybridisation,23 with faint positive lambda light chain by immunohistochemistry. Epstein-Barr Encoding Region (EBER) in situ hybridisation was negative for EBV. The staining of atypical lymphoid cells was 95% positive for Ki-67 proliferation index. B cell receptor (BCR) gene rearrangement testing using PCR confirmed the clonality of the atypical B cells. These findings were similar to those from previous biopsies of the known EC-PEL in this patient,2 thus consistent with rectal lymphoma relapse. He received doses of LD on 10 January and 7 February 2020 (table 1) and achieved remission of EC-PEL supported by rectosigmoidoscopy examination and PET scan (figure 2).
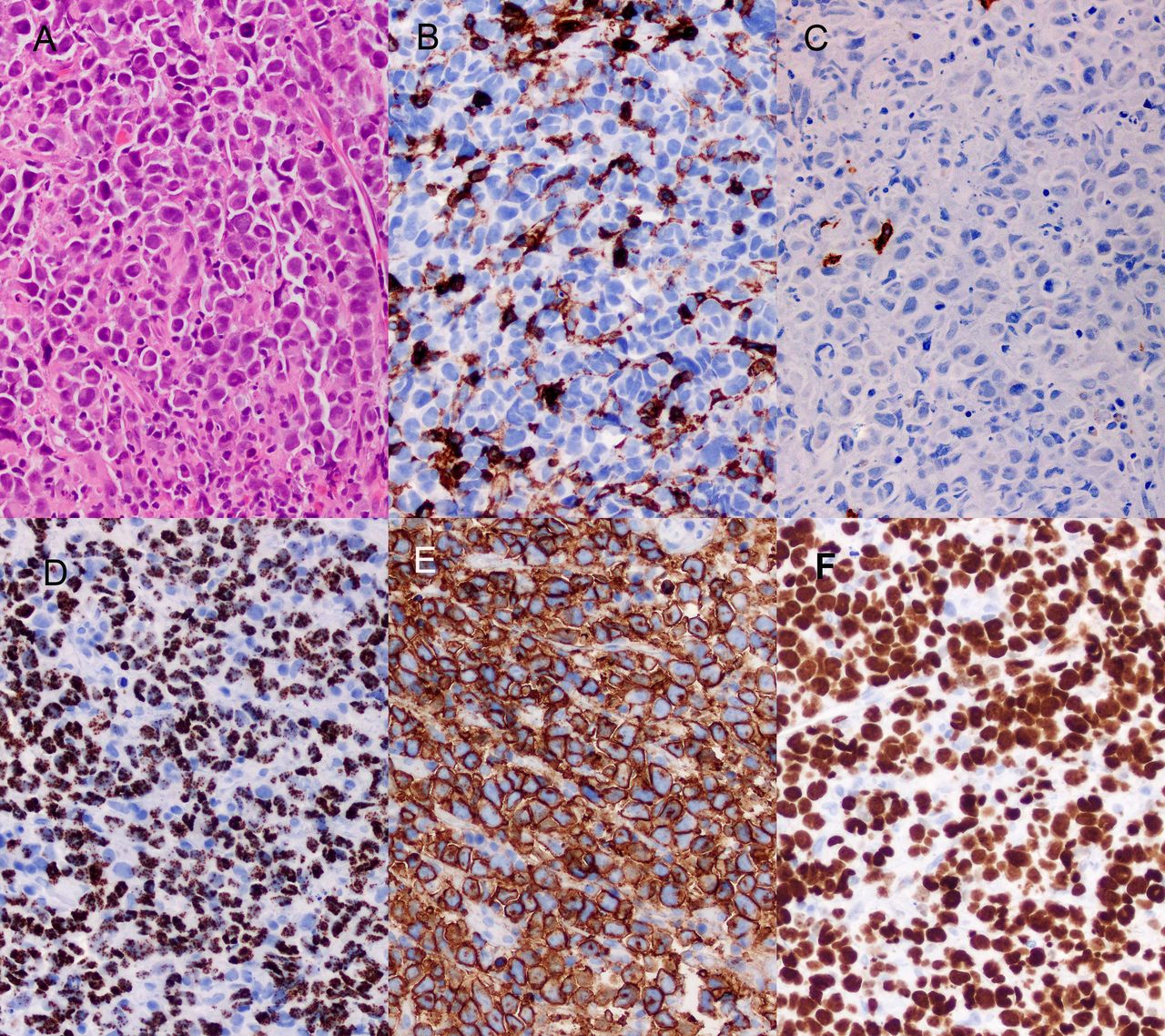
Histology and immunohistochemistry on the biopsies of the rectal mass. Medium power H&E stain showing diffuse infiltration by large atypical lymphoid cells (A). Immunohistochemistry shows neoplastic cells negative for CD45 (B) and CD20 (C), but positive for HHV8 (D) and Epithelial Membrane Antigen (EMA) (E). The Ki-67 proliferation index is very high (F). All magnifications ×200. HHV8, human herpes virus-8.

{kind=link}
{kind=link}
Images showing the mass on the rectal mucosa before and after treatment with liposomal doxorubicin infusion.
Differential diagnosis
The presumptive diagnosis of LGV proctitis was tentatively made based on the patient’s recent sexual history and presentation with rectal pain, tenesmus and fever. However, given the high RPR titre (1:128) and negative NAAT results for chlamydia and gonorrhoea, a diagnosis of syphilitic proctitis was made,24 prompting treatment with penicillin and resulting in improvement of his symptoms and a decline in inflammatory markers (table 1). Only on further investigations, including PET/CT scan, rectosigmoidoscopy and histopathological analysis of the endoscopic biopsies, the diagnosis of synchronous relapse EC-PEL was made, specifically at the site of inoculation with T. pallidum.
HHV8-positive lymphoproliferative disorders other than PEL (or EC-PEL) include HHV8-positive multicentric Castleman’s disease, HHV8-positive diffuse large B cell lymphoma and germinotropic lymphoproliferative disorder.12 Histologically, the main differential diagnosis of PEL is HHV8-positive diffuse large B cell lymphoma, but the latter usually arises in association with HHV8-positive multicentric Castleman’s disease, never present in this patient.
Treatment
The patient had been treated with ART since 2010, with persistently low CD4 T cell count (mean CD4 T cell count of 50–100 cells/mL) and with a plasma HIV viral load below the detection level (<20 copies/mL). The patient received four cycles of R-CHOP for the previous occurrence of his lymphoma and was treated with LD for cutaneous KS lesions with successful remission.2 Later recurrences of his EC-PEL in the skin and tonsils were treated with LD only, with unexpected remissions.2 At the patient’s request and to avoid second-line chemotherapy, LD was thus given between 2014 and 2017 for three recurrences of EC-PEL. The patient’s longest period of remission from lymphoma was 25 months, from September 2017 to October 2019, the last recurrence being herein reported.
Outcome and follow-up
Rectosigmoidoscopies performed on 16 January and 5 February 2020 showed rapid regression of the tumour after only one cycle of LD (figure 2). On clinical management and treatment as described above, the patient demonstrated complete clinical and tumorous response and remained asymptomatic, even on his latest visit at the clinic on 27 October 2020.
Discussion
In immunosuppressed individuals, oncogenic viruses persist in infected cells where they more effectively transformed into malignant cells. HHV8 is a DNA oncovirus that can infect endothelial cells as well as B cells and bring about the malignant transformation of both cell types. Distinct from other herpesviruses, a significant proportion of HHV8-infected cells can produce high levels of a virally encoded interleukin 6 (IL-6), contributing to inflammation and B cell extrafollicular maturation.25 When endothelial cells are preferentially infected, KS results;5 26 27 when B cells are infected,26 HHV8 creates a fertile epigenetic milieu for B cell dysfunction and establishes a pro-lymphomagenic environment, which may lead to multicentric Castleman’s disease, diffuse large B cell lymphoma or PEL. In individuals living with HIV, two or more of these conditions may develop either simultaneously or independently over time.28 Importantly, the precise diagnosis and classification of HHV8-associated lymphoproliferative disorders and KS are crucial, as their treatments and prognosis differ markedly.
PEL, a large B cell lymphoma presenting with an inflammatory syndrome, constitutes approximately 4% of HIV-related lymphomas. Whereas PEL usually presents as effusions in body cavities without identifiable tumour masses, the EC-PEL variant presents as non-cavitary masses most commonly involving the lymph nodes, skin or occasionally digestive tract. Digestive tract and mucosal involvement by EC-PEL is not common and is solely reported in a handful of cases. We reviewed the literature for these cases5 14–17 29 and included a summary of their clinicopathological features in table 2. Both PEL and EC-PEL share similar morphological, immunophenotypic and virological characteristics.3 30 The extrafollicular development of these lymphomas has been demonstrated by class-switching recombination and somatic hypermutation.25 Morphology of the malignant cells may show immunoblastic, plasmablastic or anaplastic features.2 By immunohistochemistry, they often reveal prominent features of terminally differentiated plasma cells, and the presence of HHV8 in the neoplastic cells is essential for the diagnosis. This lymphoma is also distinctive due to the common lack of expression of pan-B cell markers such as CD20, CD79a and CD19, and therefore may require BCR gene rearrangement testing to confirm its B cell lineage and clonality. CD45 expression may be low or absent, and activation markers, plasma cell markers and non-lineage-associated antigens are often expressed, including CD30, CD138 and EMA, with rare aberrant expression of T cell-associated antigens.12
HIV causes persistent immune dysfunction in B cell follicles due to the absence of T cell immune surveillance, which in turn contributes to the dysregulation of EBV latency. Therefore, as most cases of PEL and EC-PEL occur in the context of HIV, it is not surprising that over 80% of these lymphomas are associated with EBV coinfection.9 Nevertheless, cases of PEL without EBV coinfection in the neoplastic cells are occasionally reported, as in our patient, although this is most common in elderly non-immunocompromised individuals living in Eastern Mediterranean regions. Despite decades of successful ART and non-detectable HIV plasma viral load, the patient had a low stable CD4 T cell count (100×106/L) and a low CD4:CD8 ratio (0.4), indicating a reduced capacity of immune reconstitution. Interestingly, although EBV could not be demonstrated in the neoplastic cells of his lymphoma by EBER in situ hybridisation, EBV viraemia was present at the time of relapse.
One additional peculiarity of this case is that the exact date of syphilis transmission is known. In fact, the patient acquired syphilis precisely on 29 June 2019, during a single episode of receptive anal intercourse with another man, the only sexual intercourse he had over the past year, as reported. To further emphasise this, a negative RPR titre was also documented in May 2019. The patient presented 4 months after in an STI clinic in Montreal with complaints of rectal pain associated with severe constitutional symptoms and elevated inflammatory indicators, such as increased CRP, ferritin, D-dimer and β2 microglobulin (table 1). Medical history and symptomatology were consistent with syphilitic proctitis, and treatment with penicillin resulted in the improvement of symptoms, with a rapid decline in inflammatory markers. However, identification of a 5 cm ulcerated rectal mass revealed a rectal biopsy-proven recurrence of EC-PEL. The peculiar synchronous onset of rectal syphilis and rectal recurrence of EC-PEL led us to raise the hypothesis that syphilis played a role in the recurrence of this rare lymphoma.
Particularly, we speculate that the prominent inflammation induced by syphilis in the rectal mucosa may have triggered the activation of HHV8-infected B cells, favouring local development of lymphoma. As it is the case for KS, the development of PEL and EC-PEL may be dependent on sustained proinflammatory signals to render B cells more permissive to infection, subsequent activation and proliferation. In addition, using complementary in vitro and in vivo studies, mast cells have been identified as a source of proinflammatory cytokines within the tumour microenvironment.31 Consistent with this, treatment with penicillin also led to subsiding digestive symptoms and a drop in inflammatory indicators. The decline in the inflammatory microenvironment may have decreased the pro-tumorous effect of syphilis and may have increased the sensitivity of the tumour cells to chemotherapy. During the last few decades, chronic inflammation, infection, and even commensal bacteria and viruses have been reported at various extent to be associated with the development of certain Non-Hodgkin Lymphomas.23 32 33
In sum, the concomitant diagnosis of early syphilis and rectal recurrence of EC-PEL in a 59-year-old man living with HIV poses a diagnostic challenge, as both conditions may present with lymphadenopathy, skin involvement and constitutional symptoms. Rectosigmoidoscopy was key in the identification of the tumour and pathological diagnosis of recurring EC-PEL. As the development of virally induced lymphoma depends in part on the immune status of the patient, where both immunosuppression and inflammation may play a role, we consider that the syphilis-induced inflammation was a contributor to the development of the EC-PEL in this patient with low immune reconstitution. This is supported by the ‘cytokine strom’ occurring during early syphilis. Following its acquisition, T. pallidum is taken up by dendritic cells, which then trafficked it to draining lymph nodes to present treponemal antigens to naive B cells and T cells. After priming, activated T cells secrete interferon γ, enhancing the production of inflammatory cytokines, such as tumour necrosis factor and IL-6, which in this context may trigger a recurrence of EC-PEL.34 It is well established that both HHV8 and human IL-6 contribute to the transformation of infected B cells into PEL.35 Globally, IL-6 triggering, temporal association, anatomical co-localisation of syphilis and recurring EC-PEL may infer a causal or contributory role to syphilis in lymphomagenesis during HIV infection.
Learning points
Syphilis may mimic lymphoma by presenting as generalised lymphadenopathy with constitutional symptoms.
In this case report, the patient presented with early syphilis concurrently with the recurrence of extracavitary primary effusion lymphoma (EC-PEL) in the rectum, specifically at the site of Treponema pallidum inoculation.
Rectosigmoidoscopy with biopsy was key in the diagnosis of lymphoma.
Temporal association and anatomical co-localisation of syphilis and recurring EC-PEL may infer a causal or contributory role to syphilis in lymphomagenesis.
Acknowledgments
We thank the patient for his consent and help in reconstituting his complex medical history. We thank Stephane Isnard, John Lin and Brandon Fombuena for the critical review of this case report. We thank Angie Massicotte for coordination.
References
Footnotes
Contributors DSA contributed to the planning of the manuscript, reviewed the patient file, performed the literature review and wrote the first and final draft of the manuscript. MP participated in the planning of the manuscript, performed the rectosigmoidoscopies and the follow-up of the patient, reviewed the first draft and approved the final draft of the manuscript. L-AJ participated in the planning of the manuscript, reviewed the pathology aspects of the case, provided the images and their interpretation, contributed to the drafts and approved the final version of the manuscript. J-PR planned the manuscript, contributed to file review and literature review, contributed to the manuscript drafts and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.