Article Text

Statistics from Altmetric.com
- travel medicine
- tropical medicine (infectious disease)
- infectious diseases
- infection (gastroenterology)
Description
A 57-year-old man presented with a 10-day history of fever with rigours and weight loss. The fever manifested during the afternoon hours, reaching up to 39.5°C and was followed by profuse sweating. The patient reported that he had lost 7 kg during this time. He did not report any abdominal pain and on direct questioning he denied having a prodrome of diarrhoea; further, he could neither recall in his history a bout of diarrhoea lasting several (up to 6 weeks) or recurring diarrhoea over the previous years. He had been empirically prescribed ciprofloxacin and doxycycline by his primary care physician for 5 days, without the improvement of symptoms. He denied any travel to an endemic area. Physical examination was unremarkable. The liver edge was not palpable, and no tenderness was noted on palpation of the right hypochondrium.
Laboratory investigations were significant for increased inflammatory markers, specifically white cell count 12.000 cells/mL, erythrocyte sedimentation rate 66 mm/h and C reactive protein 150.8 mg/L, and a mild elevation of liver enzymes, specifically alanine aminotransferase 73 IU/L, aspartate aminotransferase 48 IU/L, alkaline phosphatase 261 IU/L and gamma-glutumayltransferase 172 IU/L.
The patient on admission was prescribed piperacillin/tazobactam, covering an extended spectrum as compared with his previous empirical antibiotic regimen, including Gram-negative, Gram-positive and anaerobic bacteria. He subsequently underwent an abdominal ultrasound, which revealed multiple confluent hypoechoic lesions without wall echoes (non-encapsulated) in the right lobe of the liver. He then underwent a CT scan, which revealed the presence of multiple confluent hypodense lesions in the right lobe of the liver (segments IV and V) which displayed reduced uptake of IV contrast. The lesions formed a multilobulated mass measuring 7.8 cm in diameter (figure 1). The patient was prescribed metronidazole 500 mg IV three times a day on a tentative diagnosis of amoebic liver abscess and continued piperacillin/tazobactam 4.5 g four times a day IV pending final diagnosis. The patient did not defervesce for 72 hours, at which point percutaneous aspiration of the abscess was requested, which was performed on the earliest available appointment on the eighth day of hospitalisation by an interventional radiologist.
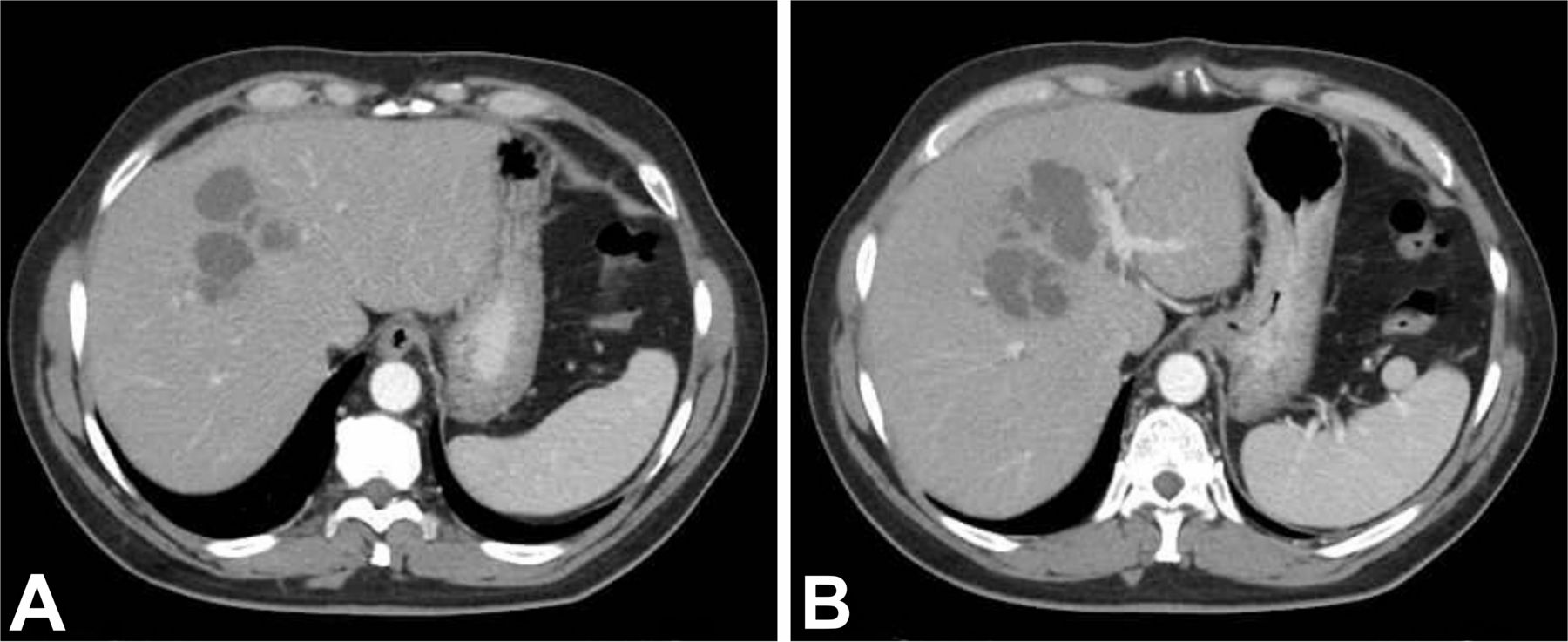
The multiple abscesses can be appreciated in the right lobe (A), which confluence near the level of porta hepatis (B) to form a multilobulated abscess.
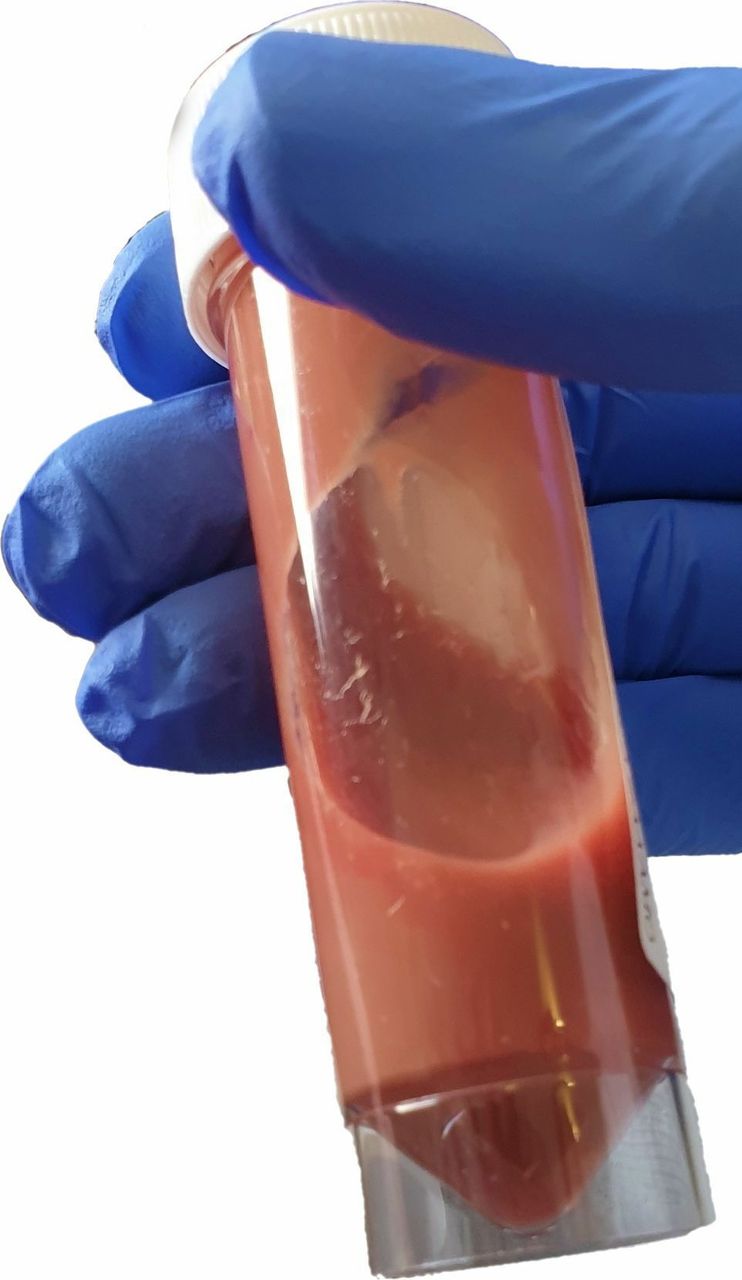
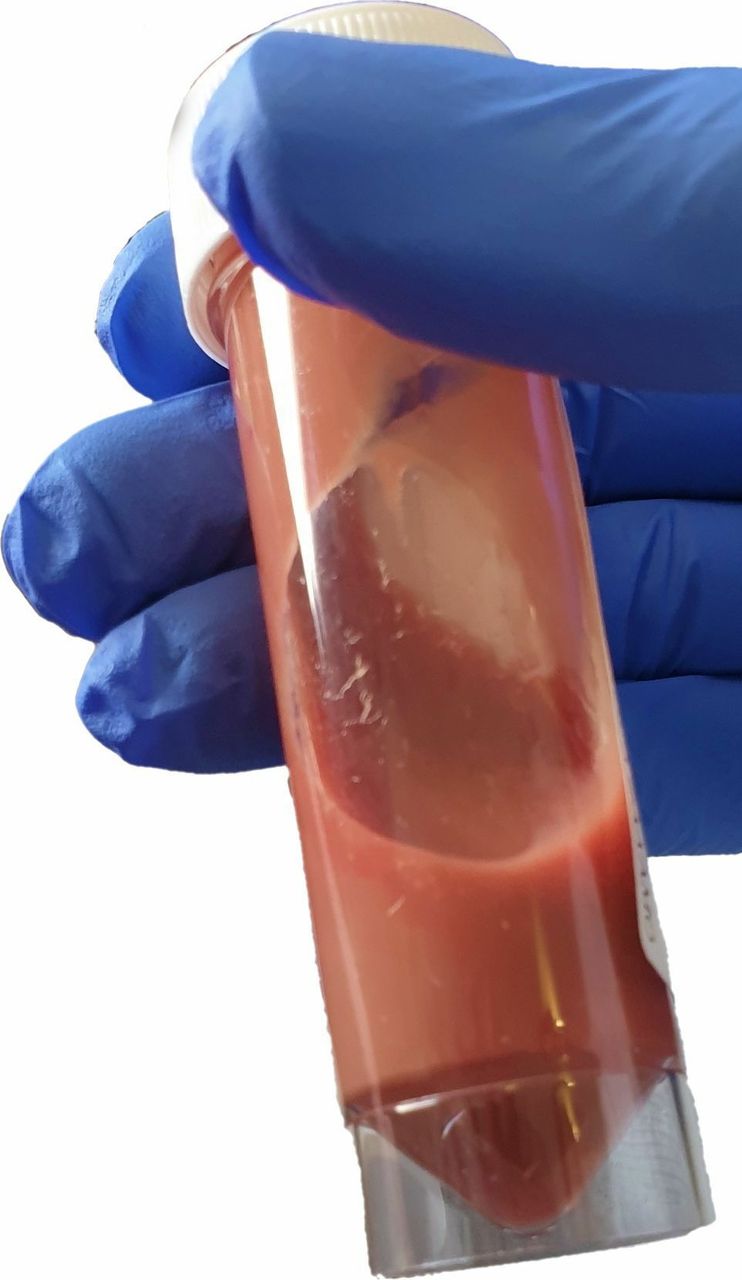
The patient underwent a CT-guided aspiration of the mass, which produced a red-brown coloured liquid (figure 2), reminiscent of the classic descriptions of the anchovy paste liquid recovered from the amoebic liver abscess. After the aspiration of the abscess, the patient defervesced within 3 days, after which piperacillin/tazobactam was discontinued.
{kind=link}
{kind=link}
A sample of the aspirated abscess fluid, reminiscent of the classic descriptions of the ‘anchovy paste’ liquid.
Cultures of the liquid were negative for the presence of bacteria, whereas direct microscopy did not reveal the presence of amoeba or other microorganisms. Stool samples taken on three consecutive days were negative for the presence of ova or parasites. Nevertheless, ELISA for antiamoebic antibodies was positive.
The patient’s condition improved, and he was discharged on metronidazole for an additional 3 weeks. Follow-up examination and CT scan 1-month postdischarge revealed resolution of symptoms and regression of the lesion, respectively.
Amoebic liver abscess usually presents as a solitary lesion. Nevertheless, early lesions can be multifocal, presenting as several micro-abscesses.1 Patients can usually be managed conservatively, with antibiotic therapy alone. However, aspiration of the abscess may be warranted either for diagnostic purposes, in cases where the diagnosis is not clear, or therapeutic purposes, such as in cases of large left lobe abscess, clinical deterioration, imminent danger of rupture or when the patient has not improved after 4 days of metronidazole treatment,2 although some authorities recommend percutaneous aspiration to be considered if there is no response after 48–72 hours, despite that response to treatment may, in fact, occur within the first 96 hours.
In our case, a luminal amoebicide such as paromomycin (indirect-acting luminal amoebicide) or diloxanide-furoate (direct-acting luminal amoebicide) was not administered, as these medications are not available on demand in our setting can only be obtained after direct import from a foreign country, after 5–7 days post prescription; our patient defervesced 9 days post metronidazole administration. Additionally, the patient on direct questioning denied having diarrhoea, did not excrete ova, trophozoites or parasites on three consecutive stool examinations and had already received 5 days of doxycycline, an indirect-acting luminal amoebicide. Had trophozoites been identified in stool, paromomycin or another luminal amoebicide would have been mandatorily administered. Metronidazole (a tissue amoebicide and to a lesser extent a luminal amoebicide) proved to be an effective treatment in our patient; metronidazole was continued until the estimated time of disappearance of the lesion, subsequently confirmed by a CT scan.
Learning points
Patients with amoebic liver abscess can present solely with fever and weight loss, whereas abdominal pain or a history of travel in endemic areas and recent bouts of diarrhoea may not be present.
Although not always warranted, in cases where antibiotic treatment does not lead to defervescence within 4 days, aspiration of the abscess can lead to resolution of symptoms.
A high degree of clinical suspicion is required for the diagnosis of an amoebic liver abscess to be made in countries in which the disease is not endemic, such as Cyprus.
Footnotes
Contributors LK: evaluated the patient, obtained informed consent and drafted the manuscript. LH: evaluated the patient and drafted the manuscript. SL: evaluated the patient and drafted the manuscript. GP: evaluated the patient, drafted and reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.