Article Text

Abstract
Stress is under-recognised as a potential causative factor for reversible cerebral vasoconstriction syndrome (RCVS). Here we present a case of RCVS occurring during a time of extreme emotional duress. A 46-year-old female patient with medical history of bipolar disorder developed a severe headache during her father’s funeral. The following day she was discovered to have bilateral hemiparesis, aphasia, encephalopathy and was brought emergently to the hospital. Neuroimaging revealed a 33 mL left fronto-parietal haematoma with subarachnoid blood near the vertex bilaterally. She underwent craniotomy, haematoma evacuation and external ventricular drain placement. The patient received two cerebral angiograms, the first showing multifocal cerebral vasoconstriction and the second showing resolution of these changes. She improved significantly over the course of her 3-week hospitalisation and eventually made a full recovery, including the ability to speak fluently in six languages with no significant deficits other than hypersomnia; she now requires 10 hours of sleep each night as compared with 7 hours prior to her brain injury.
- neuroimaging
- coma and raised intracranial pressure
- headache (including migraines)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Reversible cerebral vasoconstriction syndrome (RCVS) is a group of conditions that are caused by reversible multifocal narrowing of the cerebral arteries with clinical manifestations that can include headache, stroke and seizure.
The pathophysiology of RCVS remains unclear. Female predominance may suggest hormonal influences, particularly given the increased risk during pregnancy and the postpartum period.1 Increased sympathomimetic activity triggered by sexual activity, ingestion of sympathomimetic drugs and the increased incidence of RCVS in patients with a prior history of serotonergic antidepressant use could alternatively suggest biochemical triggers.2 3 Identification of aetiologies that could potentially lead to RCVS, such as severe emotional stress, may help to further our understanding of the pathophysiology of this disease.
Case presentation
A 46-year-old female patient with medical history of bipolar disorder presented to an outside hospital after she was found in an obtunded state by her family on the morning of presentation.
Per family, the patient developed a sudden severe headache during her father’s funeral. She was given ibuprofen, which initially helped with her headache. She described this as the worst headache of her life. Her son later gave her 1–2 tablets of naproxen which did not seem to help. She then vomited and subsequently went to bed. She had no prior history of headaches or migraines.
One day later, the patient woke up and was able to walk a few steps, but became obtunded and unresponsive shortly thereafter. Emergency medical services (EMS) were called, and she was transferred to an outside hospital. On arrival, the patient’s vital signs were blood pressure (BP): 103/84, heart rate (HR): 66 and temperature: 36.4. She was intubated for airway protection given her decreased level of consciousness.
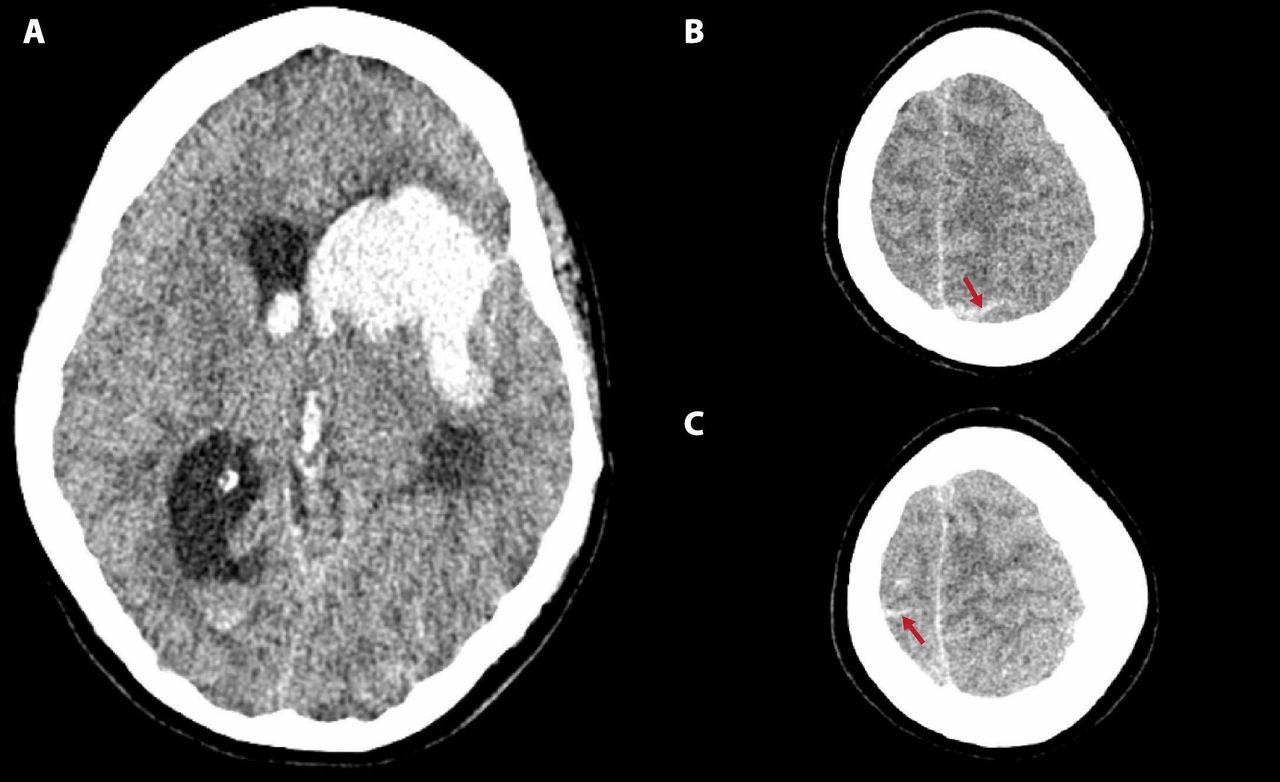
Head CT revealed a left basal ganglia/fronto-parietal haematoma measuring 33 mL in volume with mild subarachnoid haemorrhage near the vertex (figure 1). She was transferred to MedStar Georgetown University Hospital for neurosurgical evaluation. A CT angiogram of the head and neck performed on arrival showed no vascular abnormalities. The patient underwent emergent craniotomy, haematoma evacuation and external ventricular drain placement after transfer from the outside hospital. There was no history of hypertension (HTN), bleeding disorders, tobacco use or substance abuse. The patient’s only home medication was lithium, and she had been on a stable dose for several years. Family history was significant for father with Lewy body dementia.
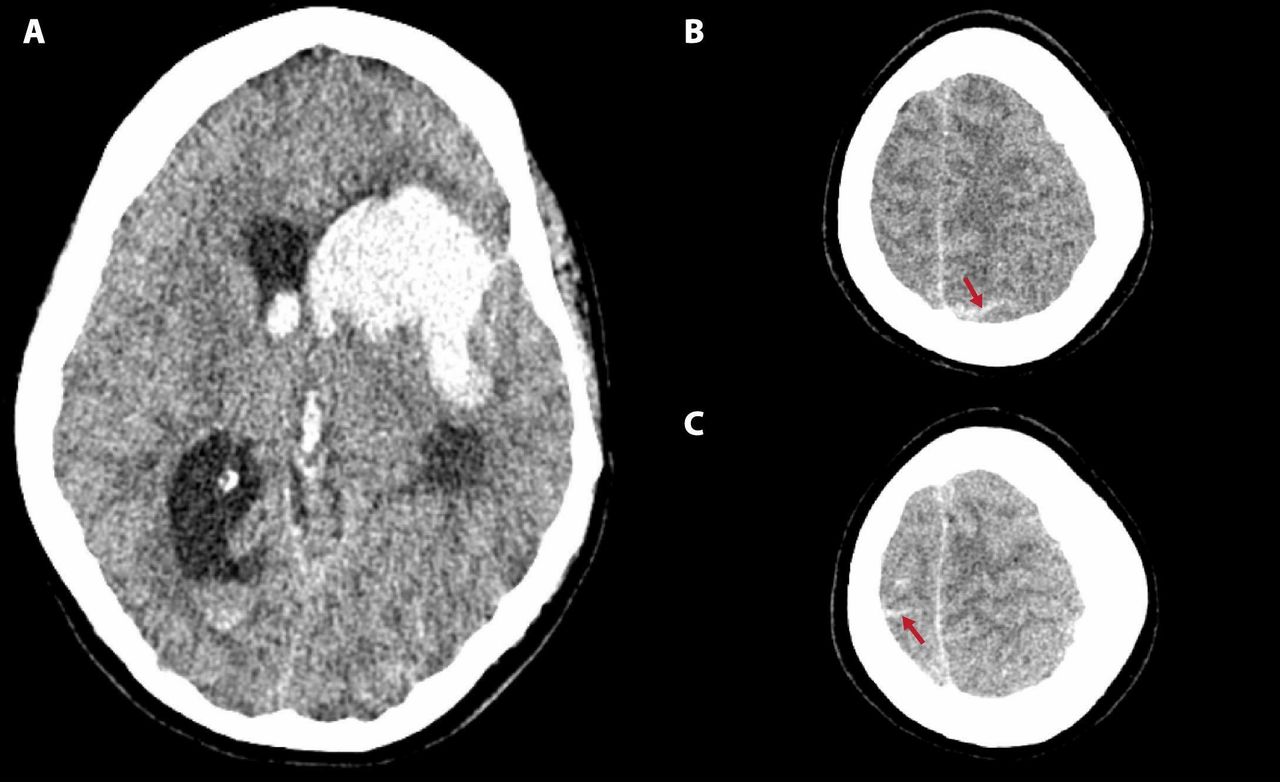
Non-contrast head CT on hospital admission. Thirty-three mL left basal ganglia fronto-parietal intraparenchymal haemorrhage with intraventricular extension (A). Subarachnoid haemorrhage near the vertex on the left (B) and the right (C) marked by red arrows.
Investigations
Cerebrospinal fluid (CSF) analysis (post craniotomy) revealed white blood cell (WBC) count : 406, red blood cell (RBC) count: 71 000, glucose: 81, protein: 223. The analysis was repeated 2 days later and revealed the following: WBC count: 14, RBC count: 2000, glucose: 84, protein: 56. Infectious workup, including CSF bacterial culture and herpes simplex virus (HSV) PCR were negative. A urine drug screen and initial lab results were all within normal limits. Rheumatological labs including antineutrophil cytoplasmic antibody (ANCA), proteinase 3 (PR3) antibody, myeloperoxidase (MPO) antibody, antinuclear antibody (ANA), erythrocyte sedimentation rate (ESR), C reactive protein (CRP), rheumatoid factor and double-stranded DNA were negative with the exception of CRP, which was elevated at 137.
MRI brain did not reveal an underlying infarct or mass; magnetic resonance venogram (MRV) of the brain showed no venous sinus thrombosis. A transthoracic echocardiogram was within normal limits.
The patient underwent two catheter-based cerebral angiograms, the first (figure 2, section A-C) on hospital day 2 revealed mild to moderate diffuse vascular irregularity with multiple areas of alternating dilatation and vasoconstriction, most prominent within the posterior circulation, especially the left superior cerebellar artery. Within the anterior circulation, these changes were most prominent in the pericallosal arteries. There was no associated intracranial atherosclerosis. A subsequent cerebral angiogram on day 16 (figure 2) showed complete resolution of the previously noted alternating dilation and vasoconstriction changes.

{kind=link}
{kind=link}
Catheter-based digital subtraction angiography of the brain on hospital day 2 (A–C) and day 16 (D–F). Panels (A) and (D) show reversal of segmental narrowing in the left superior cerebellar artery. Panels (B) and (E) show reversal of segmental narrowing in the pericallosal arteries. Panels (C) and (F) show an absent right A1 segment of the anterior cerebral artery (ACA) due to vasospasm that later reversed to show normal filling of the ACA. Areas of reversible vasoconstriction are marked by red arrows.
Differential diagnosis
Common causes of intraparenchymal haemorrhage (IPH) include HTN, trauma, cerebral amyloid angiopathy (CAA) and ruptured arteriovenous malformation (AVM). We felt hypertensive IPH was unlikely, as her systolic blood pressures were routinely in the range 110–140 with a peak of 158 during her entire hospital course and she did not have a known history of hypertension. She reported no history of trauma and there was no evidence of a scalp contusion. She was too young for CAA and the MRI showed no evidence of old microbleeds on susceptibility-weighted imaging. Neither of her catheter-based cerebral angiograms suggested an underlying AVM.
Rarer causes of IPH include cerebral sinus venous thrombosis (SVT), septic embolism leading to haemorrhage from a ruptured mycotic aneurysm, central nervous system infection such as herpes simplex encephalitis, central nervous system (CNS) vasculitis and RCVS. SVT was effectively ruled out by a normal MRV of the brain. We felt septic embolism was unlikely given her normal transthoracic echocardiogram, negative blood cultures and no fevers except for a 12 hour period during her hospital course. Despite the initial CSF pleocytosis, CNS infection was unlikely given a lack of clinical signs of infection, relatively benign CSF profile 2 days later and negative CSF HSV PCR and bacterial cultures. While CNS vasculitis can demonstrate similar areas of cerebral constriction with post stenotic dilatation on cerebral angiogram we felt this was unlikely because: (1) she had no prior history of stroke or signs of cognitive dysfunction, (2) her headache was sudden in onset which is twice as common in RCVS as opposed to the more insidious subacute headaches described with CNS vasculitis, (3) her second CSF profile showed no evidence of elevated protein or lymphocytic pleocytosis, (4) her rheumatological workup was mostly negative except for an elevated CRP and (5) her monophasic course of illness which improved with supportive treatment.4 5
Our patient met criteria for RCVS according to the recently developed RCVS2 score as well as the third edition of the International Classification of Headache Disorders (ICHD-3). The RCVS2 score was developed to accurately distinguish RCVS from non-RCVS arteriopathy including CNS vasculitis.6 Our patient’s RCVS2 score was 7—a score >5 suggests 90% sensitivity and 99% specificity for RCVS. Our patient also met all of the ICHD-3 criteria for acute headache attributed to RCVS7 including: (1) headache with focal deficits has led to angiography with ‘string of beads’ appearance and diagnosis of RCVS and (2) new thunderclap headache triggered by sexual activity, exertion, valsalva manoeuvres, emotion, bathing and/or showering with no new significant headache after >1 month. In addition to meeting the RCVS2 and ICHD-3 criteria, our patient had non-aneurysmal subarachnoid haemorrhage at the convexities, which is seen in around one-third of RCVS cases.8
Treatment
She underwent emergent craniotomy with clot evacuation followed by close monitoring in the neurological intensive care unit. She was started on oral nimodipine 60 mg every 6 hours once RCVS was suspected on angiography, which was discontinued at the time of discharge.
Outcome and follow-up
The patient’s mental status improved significantly over time. Post extubation she was intermittently confused about where she was and had a moderate expressive aphasia. Her inpatient hospitalisation lasted 20 days and her subsequent stay in an inpatient rehabilitation facility lasted around 2 weeks. Of note, the patient's job required her to speak at least two different languages—English and Chinese. In addition, the patient, prior to her brain injury, spoke six languages. Around 1 week into her hospital course she was able to speak three languages and by the time she saw speech therapy as an outpatient after discharge from inpatient rehabilitation, and at her initial follow-up, she was able to speak four languages without any deficits. One year after her brain injury, the patient was able to speak all six languages. The only change has been that she now requires 10 hours of sleep at night. She is currently back at work and able to perform all of her prior job duties.
Discussion
RCVS is known to affect younger individuals with a female predominance as in the case of our patient. RCVS has a mean incidence around age 42 years, however cases have been described from age 4 months to age 65 years.9 The most common presentation is multiple recurrent thunderclap headaches over a period of 1 week. The major complication is subsequent cerebral infarction/haemorrhages resulting in permanent residual neurological deficits.2 RCVS is characterised by prolonged segmental vasoconstriction of anterior and posterior circulation cerebral arteries seen on non-invasive or invasive angiography. RCVS demonstrates a bilateral multiple ‘string of beads’ appearance of the cerebral arteries caused by segmental vasoconstrictions and post-stenotic dilatations. RCVS is sometimes missed on non-invasive neuroimaging with computed tomography angiogram (CTA)/magnetic resonance angiogram (MRA) and may only be seen using invasive, catheter-based angiography, as in our case.9 Vasoconstriction can be symptomatic or persist after resolution of symptoms. The vasospasm reversibility must be demonstrated by an angiographic control within 12 weeks after presentation.2 Reversible cerebral oedema may also be seen in a minority of RCVS patients.
RCVS may occur in pregnancy, post partum, after exposure to drugs with serotonergic and sympathomimetic actions, trauma, HTN, migraine, hypercalcaemia, porphyria or other related conditions. There are no clinical or preclinical studies that clearly delineate the pathophysiology of RCVS, but increased sympathetic drive has consistently been described as a possible inciting factor. Circulating catecholamines are elevated in conditions like pheochromocytoma or after ingestion of sympathomimetic drugs and have resulted in secondary RCVS.10 In addition, there are multiple reports suggesting that consumption of diet pills and energy drinks containing sympathomimetic compounds have triggered RCVS. The possible inciting ingredients in these reports include green tea, L-carnitine, conjugated linoleic acid, the weight-loss supplement Hydroxycut, Chinese medicine containing ephedra and ‘energy drink’ containing numerous sympathomimetic herbal compounds.8 11–13
Stress could conceivably trigger RCVS through activation of sympathetic pathways and catecholamine surge. Physiological situations, including emotional stress, recent surgery, sexual intercourse, bathing, high altitude and others, have been reported as potential triggers of RCVS.3 One study showed the presence of cerebral vasospasm in patients with post-traumatic stress disorder.14 Two prior case reports specifically describe grief as the probable inciting factor. Fisher detailed a case of RCVS triggered when the patient’s favourite horses were taken to the glue factory.15 Ducros and Wolff later described a case in which the thunderclap headache started when a woman placed flowers on her husband’s grave during his funeral.3 Given our case and these prior examples, it is conceivable that grief is a stress-related trigger leading to catecholamine surge. Grief may be an under-recognised trigger for RCVS.
Serotonergic pathways have also been implicated as a possible trigger for RCVS. For example, a study by Noskin et al discovered a possible relationship between starting an Selective Serotonin Reuptake Inhibitor (SSRI) and the development of RCVS.16 Of note, there are no documented cases of lithium use and the development of RCVS, which was the only medication our patient was taking.
RCVS is typically managed by supportive care. Our patient was managed surgically with haematoma evacuation/external ventricular drain (EVD) placement and medically with nimodipine. Data from two case series suggested that nimodipine does not affect the time course of cerebral vasoconstriction but it may relieve the number and intensity of headaches.17 18 However, a study by Ducros et al revealed that nimodipine may not be very effective as more than 30% of patients had headache recurrences.9
In our case of RCVS, grief was the suspected trigger and likely cause of the condition. Hence to the best of our knowledge, this is one of only a few case reports of grief-induced RCVS. Prompt evaluation and early recognition of this condition can help in the management of RCVS patients. Awareness that grief could be an inciting factor may help increase early detection of future RCVS cases.
Patient’s perspective
I have no recollection of being a patient in the neurology/neurosurgery ICU for around 20 days.
I only remember waking up in the rehabilitation hospital, having been told by my mother that I had a neurosurgery due to massive bleeding in my brain because of a condition called RCVS. My last memory is of speaking about my father at our shiva service (the prayer service for the dead) during the evening of January 11, 2016; I don’t remember but I was told by my mother that I went upstairs to my bedroom, where I must have lost my consciousness that evening. The next morning, I was transported to a hospital and then to another hospital for the emergency neurosurgery on 12 January 2016.
I do remember that the date of my father’s funeral service, 10 January 2016, was one of the most emotionally painful days of my life. I also remember exactly when I got my thunderclap headache, which was about half an hour before the funeral service for my father started. It was the most painful, throbbing headache I have ever experienced; I am amazed that I was able to speak at my Dad’s funeral service and recite a poem on him, and that I was able to lead his burial that afternoon—even with the most painful headache ever. How lucky am I that today I can do everything I could do then, with the exception that I now sleep 10 hours daily!
I feel a depth of gratitude to my amazing neurosurgeon, who saved my life, along with all doctors, nurses, and other hospital personnel, who took care of me in the ICU that I have been able to make a full recovery.
I was glad to be a neurology/neurosurgery Grand Rounds patient at the 30 March 2017 Grand Rounds presentation. Having this article published also will hopefully help others dealing with RCVS. Having my life saved has inspired me to want to help others. There are really no words to describe the extent of my gratitude for surviving such a dangerous life-death situation.
Learning points
Reversible cerebral vasoconstriction syndrome (RCVS) is a group of conditions characterised by reversible constriction of cerebral arteries.
Most patients present with a thunderclap headache.
Approximately one-third of patients develop ischaemic or haemorrhagic strokes or reversible brain oedema on neuroimaging.
Emotional stress and grief, based on our case could be a potential trigger for RCVS.
References
Footnotes
Twitter @poojara52867811
Contributors PR: she was involved in planning the write up and additional data acquisition. She was also the point of contact for the patient in obtaining follow-up information and consent. MFM: he helped acquire accurate images of the patients angiogram and CT head during hospitalisation. JS: she was involved in editing the article and providing data in the discussion section with important feedback which was helpful. MAE: he was involved in the conception and design of the case report. He made sure all the data were presented in a succinct and precise manner.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.