Article Text

Statistics from Altmetric.com
Description
A 57-year-old woman with bullous emphysema and very severe airflow limitation with a forced expiratory volume in the first second of 18% predicted, presented to an outside facility with worsening cough, sputum production and shortness of breath. She had been hospitalised multiple times in the last 6 months and was intubated twice for acute exacerbation of the chronic obstructive pulmonary disease. She had more than a hundred pack-year history of smoking and quit 6 months earlier. On admission, she was tachypneic, tachycardic and short of breath. Chest auscultation revealed diffuse rhonchi and distant breath sound bilaterally. An arterial blood gas demonstrated acute on chronic hypercapnic respiratory failure, and she was started on non-invasive positive pressure ventilation with some improvement in her respiratory status. She also received intravenous steroid, azithromycin.
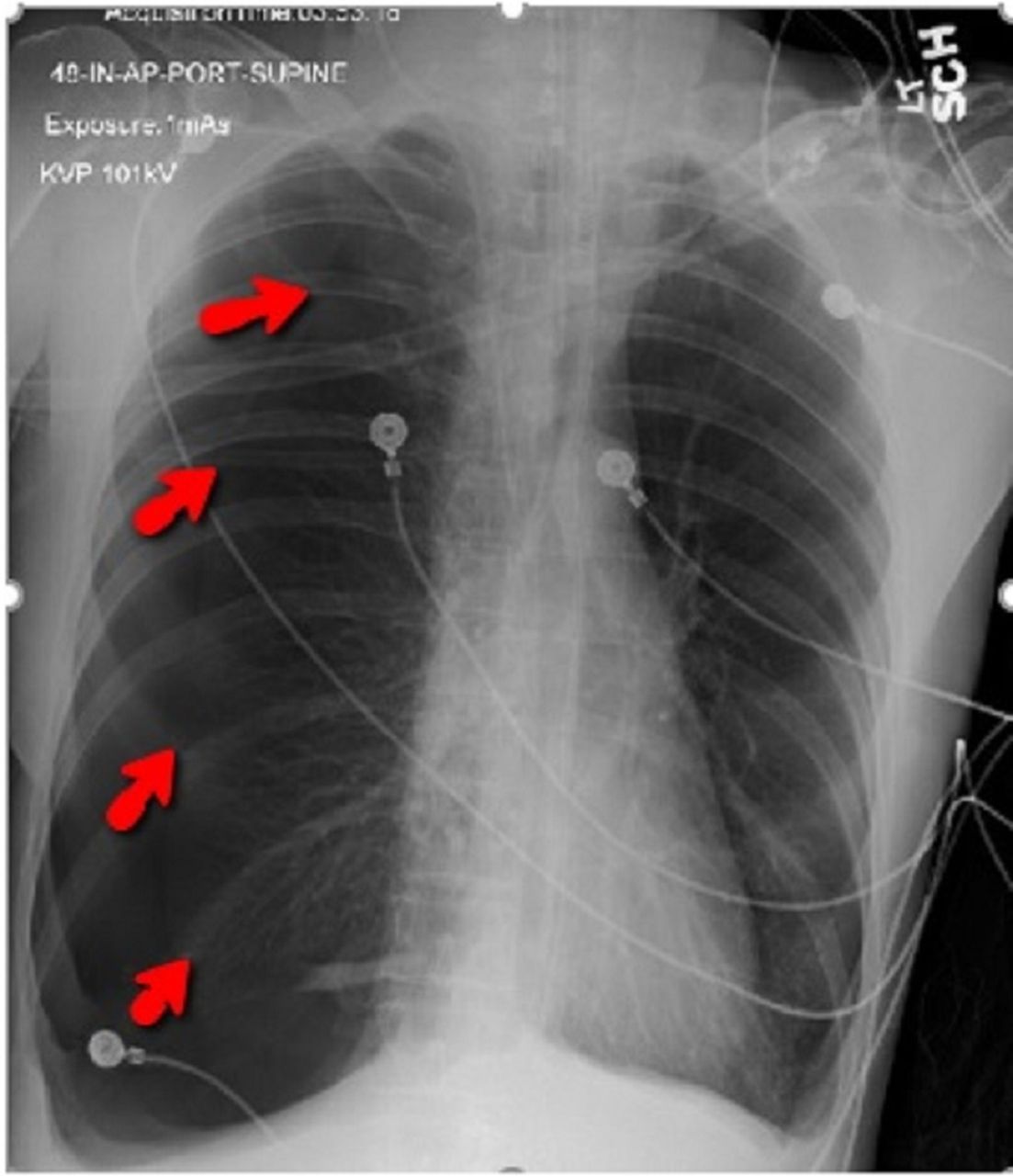
Eighteen hours following the admission, she became unresponsive due to worsening hypercapnia. She was intubated and started on mechanical ventilation. A right internal jugular central venous catheter was inserted. The patient soon became hypotensive and tachycardic. Fluid resuscitation was initiated. Chest X-ray is shown in figure 1. She suffered from cardiac arrest with pulseless electrical activity. Following a brief period of cardiopulmonary resuscitation, resumption of spontaneous circulation was obtained.
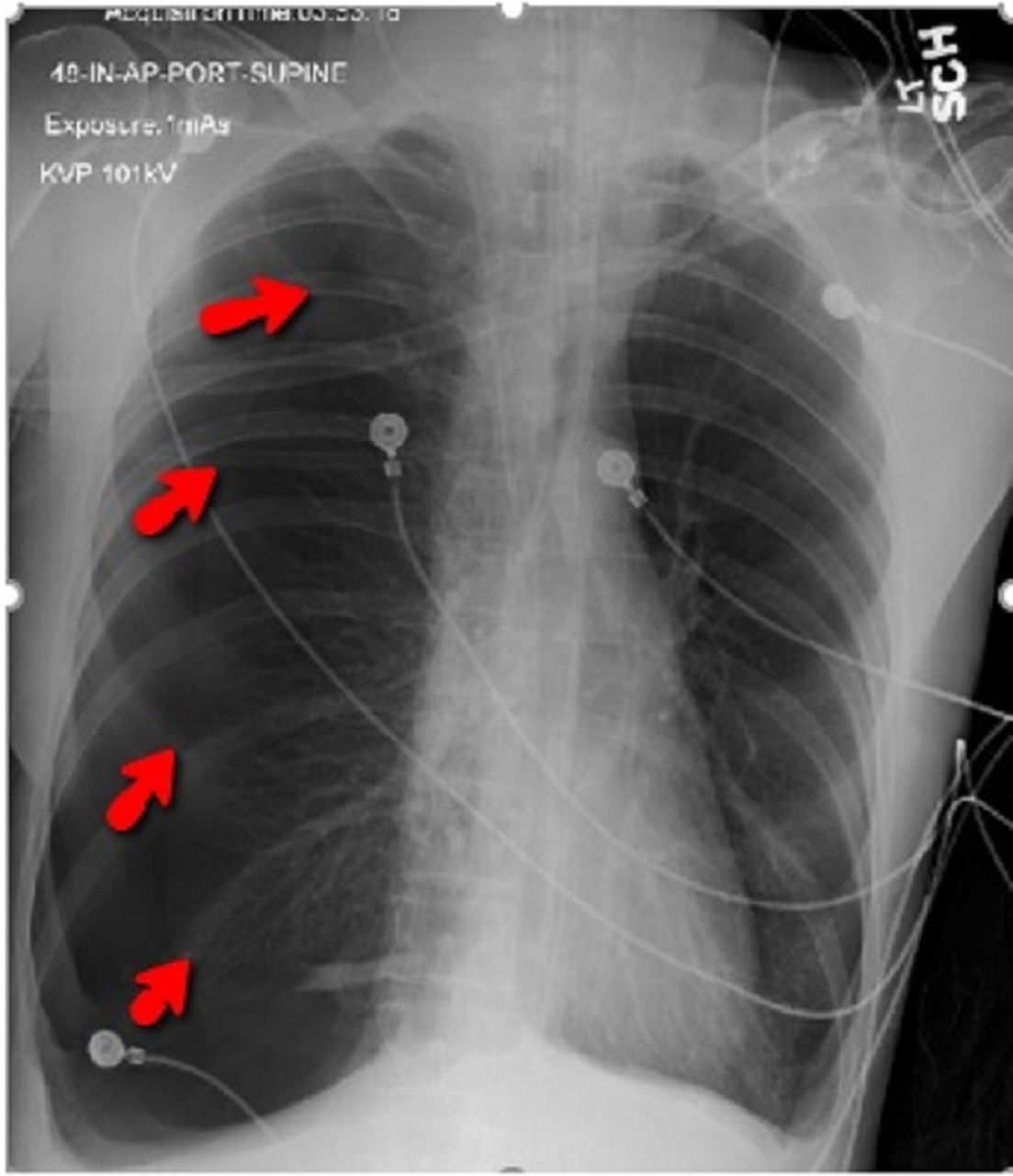
Chest X-ray showing large right-sided tension pneumothorax with collapsed lung margin (arrow).
An emergent needle thoracostomy was performed, followed by the insertion of a small-bore chest tube (SBCT) (18 Fr). A large air leak—with a difference of about 250 cc between inhaled and exhaled volume—was noticed. Over the next 2 days, the patient developed worsening subcutaneous emphysema (SE), and the chest tube suction was increased to 30 cm of water without any benefit. The patient was subsequently transferred to our facility.
On arrival to our institution, the positive end-expiratory pressure was reduced to 0, and pressure support ventilation was initiated. The air-leak persisted (~120 cc). The SE deteriorated and involved her entire body with a grade 5 SE.1 No pneumothorax was visible on multiple chest roentgenograms (figure 2). Due to clinical failure of the SBCT, a 32 Fr or large-bore chest tube was inserted.2 CT scan following the chest tube insertion is shown in figure 3.

Chest X-rays performed on day 3 (A) and day 5 (B) demonstrating worsening subcutaneous emphysema without any evidence of pneumothorax.

{kind=link}
{kind=link}
{kind=link}
(A) Chest X-ray following insertion of 32 Fr chest tube. (B) Axial chest CT showing moderate right pneumothorax, subcutaneous and mediastinal emphysema. (C) Sagittal view with profound SE of the entire length of the radiographic field. (D) Partial re-expansion of the right lung with the chest tube lodging in the right major fissure. SE, subcutaneous emphysema.
Over the next few days, SE completely resolved. Tracheostomy was performed due to end-stage lung disease from emphysema. The chest tube was successfully removed.
Learning points
A small-bore chest tube (SBCT) (18 Fr or smaller) is usually adequate to treat pneumothorax and commonly used in practice due to the ease of insertion, as well as better patient tolerability. However, persistent and worsening pneumothorax, or subcutaneous emphysema (SE) following insertion of an SBCT might be an early indication of failure to adequately drain the pleural space in patients with tension pneumothorax, especially in the presence of structural lung disease, iatrogenic pneumothorax and mechanical ventilation.
Absence of pneumothorax on a supine chest X-ray does not definitively rule out the possibility. The chest X-ray has low sensitivity for identification of pneumothorax, and a CT scan might be needed to identify, and adequately three-dimensionally quantify the pneumothorax. A false-negative chest X-ray is more likely in patients with partially reinflated lung. The occurrence of worsening SE in the absence of pneumothorax on chest X-ray in this patient led to delayed recognition of SBCT failure and contributed to patient morbidity. Although rarely life-threatening, SE is often anxiety-provoking for the patient’s family.
A large-bore chest tube should be inserted at the earliest sign of SBCT failure.
Footnotes
Contributors BKS and SB took care of the patient. BKS was involved in planning and data acquisition. BKS and AS prepared the initial manuscript. SB supervised the final preparation of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.