Article Text

Abstract
We describe an 11-year prospective clinical and radiologic course of a 6-year-old boy with bilateral Legg-Calvé-Perthes disease, who was treated with intravenous pamidronate (IV-PAM). His baseline radiographs showed grade IV avascular necrosis/Catterall stage IV, and at worst he progressed to lateral pillar/Herring stage C bilaterally. His disease initially was extremely functionally limiting with expected poor outcome with eventual joint replacement. Because IV-PAM stops bone breakdown and allows for ongoing bone formation while revascularisation of bone occurs, we hypothesised that IV-PAM could act as an adjunct to traditional treatment to help heal the femoral heads. Our patient received nine once monthly doses of IV-PAM (1 mg/kg/dose) over 13 months, along with Petrie/broomstick casts and physiotherapy. Remarkably, over time, his femoral heads healed. Now, at 11-year follow-up, he has excellent functional and radiologic outcome with congruence between femoral head and acetabulum, no residual osteonecrosis and minimal loss of femoral head sphericity.
- Paediatrics
- Orthopaedics
- Therapeutic Indications
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Legg-Calvé-Perthes disease (LCPD) presents in childhood with idiopathic avascular necrosis of the femoral head(s), which can lead to disability and the requirement for corrective surgery at a young age. The disease has four chronological stages: (1) initial, (2) fragmentation, (3) reossification/healing and (4) residual/healed.1 Progression through these stages can last from 4 to 6 years, and is longer for older patients.2 3
The pathophysiology of LCPD is still not completely understood.3 There exist few nonsurgical treatments that modify the disease course.4 5 In general, those with worse (>50% femoral head) involvement tend to be treated surgically with an osteotomy, which is a major surgery.6–8 A poor prognosis is indicated by greater spherical incongruency between femoral head/acetabulum at skeletal maturity,9 a greater extent of necrosis, bone age >6 at diagnosis,10 11 excessive stiffness11 and reduced range of motion.12
Recently, there has been increasing evidence for the use of bisphosphonates in treating LCPD.13 Bisphosphonates are a class of drugs that prevent the osteoclastic resorption of bone.14 In humans, there are few published reports including one case report and one case series of the use of a bisphosphonate, zoledronic acid (zoledronate), in LCPD,15 16 and a clinical trial for zoledronate in LCPD is currently underway.17 Pamidronate (PAM) is a second generation bisphosphonate, for which there are no reports of use in LCPD, but which has been beneficial in paediatric patients with inflammatory bone diseases, such as chronic for chronic recurrent multifocal osteomyelitis (CRMO), in osteogenesis imperfecta and in malignancy-related bone morbidities.18–20
This paper provides a case report and pictorial essay illustrating the course of a boy who presented with bilateral LCPD at age 6 years, was treated with a course of intravenous pamidronate (IV-PAM) and was prospectively followed for 11 years.
Case presentation
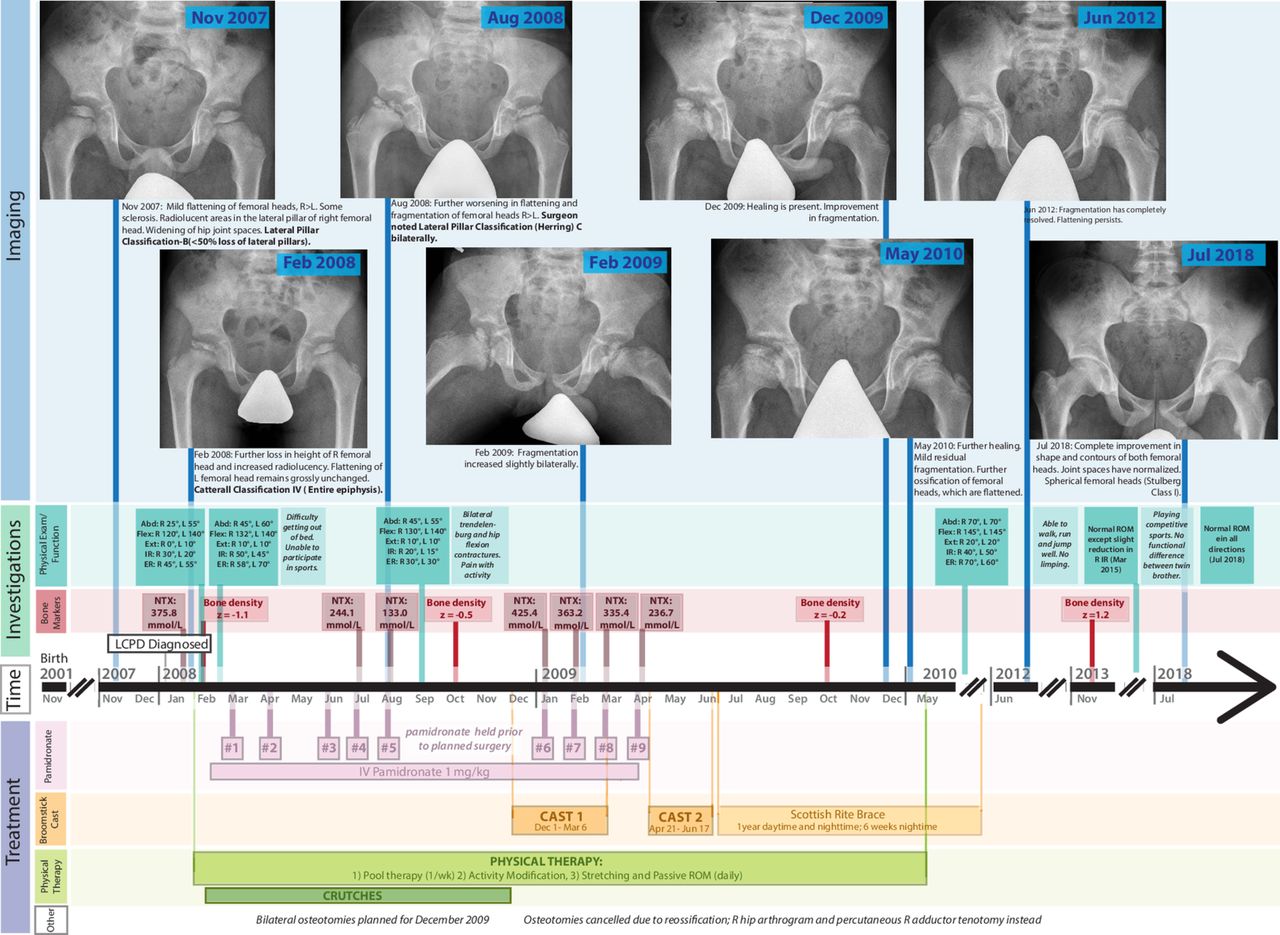
Our patient was born as a twin via emergency caesarean section in November 2001. He was born 3 weeks prematurely due to pre-eclampsia after a pregnancy complicated by gestational diabetes. At age 6 years (June 2007) his parents sought medical attention for progressive right hip pain and occasional left hip pain. In November 2007, the diagnosis of LCPD was confirmed, based on clinical presentation and imaging, by the treating orthopaedic surgeon (CB). By August 2008, he had received five IV-PAM injections. At this point, his imaging was consistent with grade IV avascular necrosis, stage IV Catterall classification and lateral pillar classification stage C bilaterally (figure 1).

Timeline of the patient’s treatment and investigations. X-ray images are cropped to focus on the hips and are labelled by date. Abd, abduction; ER, external rotation; Ext, extension; Flex, flexion; IR, internal rotation; L, left; NTX, N-telopeptide; R, right; Z, Z-score.
Investigations
The physical examination results alongside relevant imaging for the patient’s time course in care are shown in the pictorial essay and timeline (figure 1).
Treatment
Pamidronate
Because of anticipated poor outcome with need for surgery and eventual joint replacement, IV-PAM treatment was initiated. He received 9 courses of IV-PAM (1 mg/kg/month) from March 2008 to April 2009 (it was stopped from September to December 2008 prior to planned osteotomies, which were cancelled due to an excellent response to PAM with reossification of his femoral heads, figure 1). He received calcium 500 mg and vit D 400 IU supplementation daily during this time. His bone density (DEXA) and N-terminal telopeptide (NTX) were measured during administration of IV-PAM (figure 1).
Casting and bracing
During the first 4 months of IV-PAM, we initially felt that IV-PAM had not been enough, as the grade of AVN worsened radiographically. Radiographic images from August 2008 (figure 1) display the peak of the patient’s disease. At this time, he had received five injections of IV-PAM. Initially, as the patient continued to decline and due to bone loss displayed in the radiographs (figure 1), he was booked for bilateral femoral osteotomies; the exact type of osteotomy (valgus, varus or derotation) was to be determined in the operating room. During the 3 month presurgery wait time, IV-PAM was held. Unexpectedly, the radiographs performed on the day of planned surgery revealed rapid and significant improvement of the femoral heads. In December 2008, it was determined that his femurs had progressed from the fragmentation stage (stage 2) into the reossification stage (stage 3), and osteotomies were cancelled. Using a right hip arthrogram in the operative suite, the surgeon (CB) found that the right femoral head could be contained with an adductor tenotomy, so the major femoral osteotomy surgery was revised to minor adductor tenotomy.
Petrie/broomstick casts were applied to improve function, for 21 weeks total (13 weeks from December 2008 to March 2009 and 8 weeks from April 2009 to June 2009). After the casts were removed, the patient was put into a Scottish Rite brace for 1 year (which he wore as much as possible; figure 1). For the final 6 weeks of bracing it was worn only at night-time and then completely removed. At this point the patient was 8 years old, and reported no pain.
Physical therapy
The patient received physical therapy throughout his entire course of treatment. This was most intensive prior to being fitted into the Petrie/broomstick casts, and consisted of activity modification, daily at-home stretching exercises (passive range of motion (ROM)) and once-weekly pool therapy (figure 1).
Outcome and follow-up
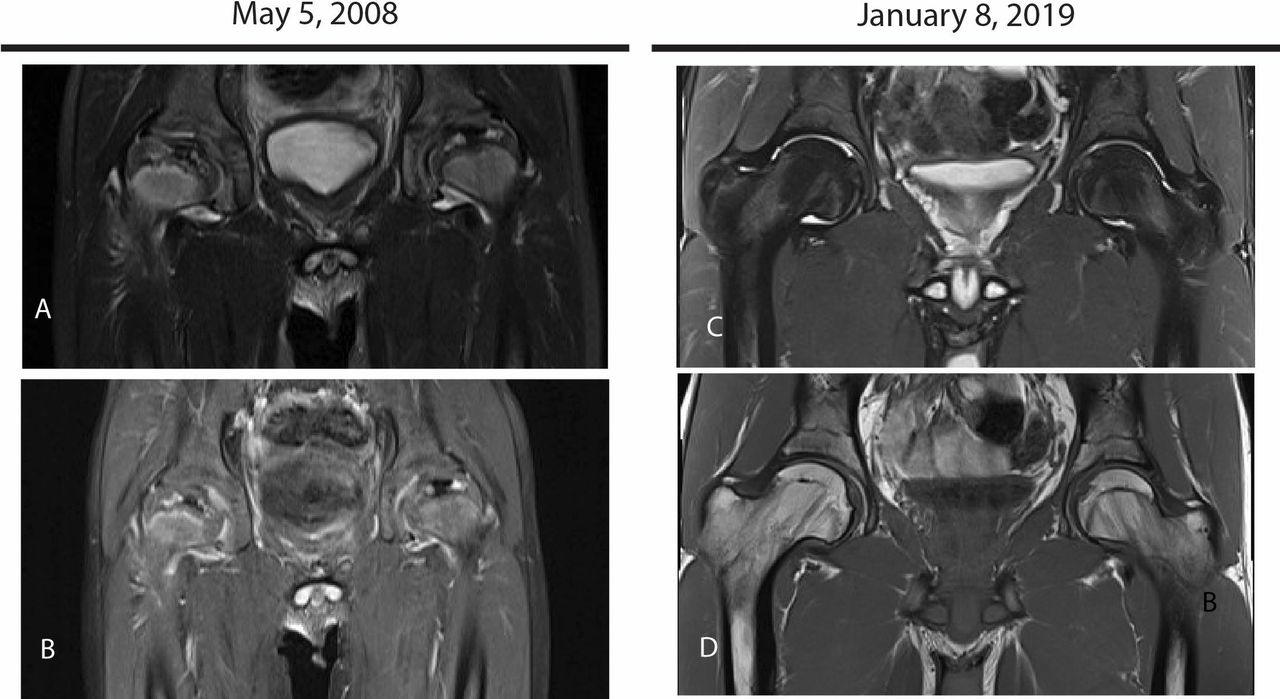
By May of 2009 the patient was pain free (figure 1). He gradually returned to sports and by 2015 he was playing competitive soccer with no functional limitations. In 2016, his family noted that there were no functional differences between him and his twin brother. The patient’s radiographic images from 2016 showed slightly flattened bilateral capital femoral epiphysis with a mild coxa manga deformity. In 2018, radiographic images showed complete improvement in shape and contours of both femoral heads, with normalised joint spaces and Stulberg class I (classification scale for LCPD relating to spherical congruency of the hips, with Stulberg class I indicating normal congruency,9 12 figure 1). MRIs of the patient’s hips during IV-PAM treatment, and 11 years later are shown in figure 2. His MRI at age 17 showed marked improvement in his previously fragmented femoral heads, with no residual avascular necrosis and minimal loss of sphericity.
{kind=link}
{kind=link}
A comparison of the patient’s MRI scans in May 2008 (A, B), at the peak of his disease, and in January 2019 (C, D) at 11 year follow-up. (A, B, 2008): Coronal Short T-1 Inversion Recovery (STIR) (A) MRI demonstrates fragmented appearance of right femoral head which is markedly flattened. Mild flattening of left femoral head. Mixed high and low signal intensities in both femoral heads with central low signal areas suggestive of necrotic areas. Coronal T1FS post-gadolinium (B) additionally reveals minimal enhancement throughout the femoral heads, particularly along the lateral pillars. (C, D, 2019): Coronal STIR (C) of bilateral hips and coronal T1 of bilateral hips (D) show marked improvement in previously seen fragmented femoral heads. No residual avascular necrosis is present. There is minimal residual loss of sphericity. No abnormal joint effusion(s) are present.
Discussion
We have provided an 11-year follow-up of a 6-year-old boy who presented with severe LCPD and was treated with nine once monthly treatments of 1 mg/kg of IV-PAM, a second-generation bisphosphonate, in addition to two periods of Petrie/broomstick casts and ongoing physiotherapy and who had an excellent functional and radiological outcome. There are limited studies on the use of bisphosphonates in LCPD, all of which to our best knowledge are described in table 1.
Description of previous studies examining the use of antiresorptive agents in children with LCPD
LLegg-Calvé-Perthes disease .
Dosing and choice of bisphosphonate
Table 1 summarises all published literature regarding bisphosphonates in LCPD. Even 11 years after our patient’s IV-PAM treatment, there is only one pending clinical trial examining the use of bisphosphonates in LCPD that is yet to be completed (table 1).17 Only one previous case report has reported on pain, bone density and also on radiologic outcome of the hip after bisphosphonates.15 Similar to our case, McQuade and Houghton,15 demonstrated positive radiographic, pain, and functional outcomes after bisphosphonates in a 6.5-year-old boy (table 1). All previously published studies that have investigated bisphosphonates in LCPD used zoledronate (table 1).15–17 While zoledronate is a stronger bisphosphonate than PAM , it is still not widely indicated for use in children and it is not easily available. At the time our patient presented, our group had been successfully using PAM to treat children with bone pain from CRMO.20 Also, the use of PAM had been established as safe in paediatric and adult population in CRMO,20 21 chemotherapy-associated osteonecrosis, bone malignancy, osteogenesis imperfecta22 and paediatric osteoporosis (either primary or secondary to illness, medications or neuromuscular disease).23 Our decision to use PAM was based on (1) our familiarity with the drug and (2) PAMbeing the only bisphosphonate available for use in children in Canada at the time.20 The dosing regimen we chose for PAM follows that reported in a Cochrane review from 2007, the year prior to our patient beginning his PAM therapy.23 Regarding potential side effects following bisphosphonates, there are concerns about decreases in calcium postinfusion,15 and, in adult patients, there have been concerns for possible osteonecrosis of the jaw.24 There is excellent safety data regarding bisphosphonates in paediatric patients from osteogenesis imperfecta literature, and this complication has not been reported in paediatric patients during over 50 years of use.20 We have previously published guidelines for prePAM workup and recommendations for dental interventions.20 Of note, approximately 50%–60% of patients who receive PAM will have an acute phase reaction that consists of fever, myalgia and bone pain which typically occurs with the first dose only and resolves within 24–48 hours with simple analgesic support.20
Effect of PAM
We trust that in our patient, the adjuvant use of IV-PAM with physiotherapy, casting and adductor tenotomy lead to resolution of his bilateral LCPD. While casting/bracing and physiotherapy were also applied, the review of literature suggests that these interventions alone will not alter natural history. Our patient’s broomstick/Petrie casts were applied in a window that has been previously suggested to be most beneficial for patients with LCPD.25 However, literature suggests that there is little evidence that either bracing or physiotherapy modify the natural progression of disease in LCPD,5 6 with no differences in outcome compared with ROM exercises.5 Regardless of physiotherapy or bracing, it has been suggested that children will either improve spontaneously, or in severe LCPD, they will require an osteotomy based on the natural course of their disease.5 In the present patient’s case, his physical exam and radiologic findings suggested a poor prognosis, headed towards bilateral osteotomies.12 However, the planned major surgery with femoral head osteotomies was changed to minor adductor tenotomy after significant bone healing during PAMtreatment.
With PAM therapy, our patient showed improved bone density for his age (Z-score; measured by DEXA), despite being largely non-weightbearing. His urinary N-terminal telopeptide/urine creatinine ratio (marker for bone breakdown), decreased as expected with PAM, recovered when PAM was held, and decreased as expected with further PAM, in keeping with reduced bone breakdown during bisphosphonate treatment. The age-specific and sex-specific norms have been previously published.20 Similar to other reports on analgesic effects of PAM,20 our patient’s pain rapidly improved after IV-PAM was initiated, allowing him to participate in age appropriate activities with his family and peers. Rapid pain relief after bisphosphonates is attributed to bisphosphonates changing the local bone environment.20
Eleven years after his treatment, our patient has not experienced any adverse effects from treatment, and has superior functional and radiologic outcome. His anticipated outcome without bisphosphonates would have included bilateral osteotomies, potential hip replacement surgeries in future, and poor functional outcome. We anticipate the results of the current clinical trial of zolendronate,17 with interest. Based on our experience, we would recommend PAM as an important adjuvant to physiotherapy and casting, with or without adductor tenotomy, to help improve the outcome of this disabling bone condition of childhood, especially when poor prognostic factors are present.
Patient’s perspective
I am writing as a parent of the boy described in this case report. My son has a twin brother, and they both started playing soccer at age 5, they were going on full day hikes in the mountains and everything was normal. Then, gradually, things started changing for my son during his fifth year. At times, we would notice a change in his mood, he would want to take more breaks during hikes, be less inclined to do sports. This progressed until we noticed that he was limping and he would complain, saying that his legs ‘were hurt’. This is when we took him to the family doctor. We were given an X-ray requisition and we decided to do it at the local Children’s Hospital. A week later, our family doctor wanted to see us and we learnt that our son was showing symptoms of the Perthe’s disease. We were given a referral to see a specialist at the Children’s Hospital.
We never heard about this disease before and were worried when we learnt what it was. They told us that he would need crutches to remove some weights on his hips and to restrain physical activities to minimise impact. He had the disease on both hips. He could barely lift his legs to the side as the ball of his hip joint was not round anymore. His bone density was very low. They told us that eventually the blood would come back to the hip bone and the bone would grow again but for the moment, it was weak and very fragile. Any jumping, weight, impact would make his situation worst. It was really hard to tell a young boy usually really active to sit down and not move. Especially when you have a twin brother who just wants to play with one another.
The next few months were mostly physiotherapy. Once a week at Children’s Hospital and every day at home. Our son had lots of pain and inflammation from his hip joints and was very stiff. His situation was not really good and the paediatric orthopaedic surgeon at the Children’s Hospital told us that our son would likely need a surgery and be in a wheelchair (temporary or longer, we did not know).
The surgery was supposed to take about 5 hours and consisted of cutting the head of the femur, to reposition it at an angle and have pins to keep everything in place. In the meantime, we also met with a paediatric rheumatologist in rheumatology who proposed to try a medicine (PAM) to improve our son’s bone healing. She explained that it was used for other bone diseases and that our son could possibly benefit from it. Our son was one of the first patients to try this medicine for Perthe’s disease.
We wanted to give our son all the chances so we decided to try the PAMe. The first time he received the medicine, he was not feeling very well and had fever and achy bones, but it was what our paediatric rheumatologist had explained to us could happen with the first dose. He was not sick after the subsequent sessions. On the morning of planned orthopaedic surgery, the orthopaedic surgeon took some X-rays to have a better idea of what they will find during the operation. After looking at the X-rays the doctor came back saying that it was like a miracle, our son’s bones were already healing very well and there was no need for the big surgery anymore. He only had a 30 min surgery to slightly cut the muscle in his groin to improve his flexibility and to be able to put him in a broomstick cast. It was fantastic news!
I remember the same day of the surgery they had a movie in the evening at the hospital and the nurse came asking our son if he wanted to watch the movie. He was feeling good enough to go but could not really move. The nurse said that it was not a problem, they took him on the bed and rolled it to the theatre. The movie was Happy Feet, which was a little bit ironic with a boy in a cast from toes to hips. We spend a good time, mom and son, enjoyed the movie and could relax after the stress of the day.
Our son spent about 6 months in his broomstick cast (3 times 2 months). I was impressed how wide his legs were apart as with the broomstick cast—he was larger than the elevator door at the hospital. He was mostly moving in a wheelchair but also with crutches or even on the floor with his arms. His physiotherapist at the hospital did a video of our son to show other kids who eventually will be in a similar situation how they can move and go from the floor to their crutches or wheelchair and vice versa.
Our son had the chance to have his cast done with a broken hockey stick from one of the Calgary Flames hockey players instead of a regular broomstick. We even went to a Flames game, got an autograph from the same player, a tour of the Saddledome and an interview with a journalist at Radio-Canada. Having a positive attitude and nice surprise like this one is all part of the healing process and it helps a lot.
After 6 months in a cast, our son had to relearn how to walk and rebuild his muscles. He had to use a brace to maintain his legs apart. We went for multiple years every week to physio appointments in the pool at the Children’s Hospital. Our son loved it. With a hospital looking like a Lego construction he was never afraid and never complained about his multiple appointments. He received excellent services and treatments from everyone.
Swimming was a good sport for our son as it has no impact on the joints. We were explained that the more he moved, the more the blood flowed and helped the bones grow again. He did all his swimming classes and he is now a swimming instructor and lifeguard.
In summer 2010, our son was so happy to be able to play soccer again (with his brace). At around 10 years old, 5 years after he started to have pain to his hips, he could gradually remove his brace and move as much as he wanted. His legs were maintained apart for so long that it took him another 2 years to be able to run properly and not look like someone who tries to run after doing a horse ride.
Our son is now 17 years old, plays Soccer Tier II and runs as fast as his twin brother. He even registered for his first half marathon which will be in May 2019. I’m very proud of him and his positive attitude. Our son is very grateful of all the fantastic treatments and services he received. He even did a presentation about the Perthe’s Disease in his Biology class and his experience gave him an idea of what he would like to do for living. He is already accepted into the University of Calgary in Engineering and is planning to be a Mechanical Engineer, specialising in biomedical engineering.
Learning points
Severe Legg-Calvé- Perthes disease (LCPD) can have poor long-term outcome and need for potentially multiple joint replacements during a patient’s life.
No standardised medical treatment for LCPD exists.
Bisphosphonates, such as pamidronate (PAM), temporarily stop bone breakdown while allowing continuous bone formation and increase in bone strength (bone density).
PAM appeared to accelerate time to reossification in this patient with severe LCPD and resulted in remarkable bone healing and normalisation of function.
Our results suggest that pamidronate may be considered as an adjunctive therapy for LCPD, with a goal to optimise long-term clinical, functional and radiologic outcome and to avoid femoral osteotomy.
References
Footnotes
Contributors PMM was the senior author who conceptualised the prospective treatment course with pamidronate and was the physician responsible for medical care of the patient. SH was responsible for analysing the prospective radiologic images of the patient. CB was responsible for the orthopaedic care of the patient and coordination of non-medical management (physiotherapy, braces) and functional assessments. LL was the medical student involved in the project and she and PMM drafted the original manuscript with input from all authors. All authors provided critical feedback and contributed and approved of the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Parental/guardian consent obtained.