Article Text

Statistics from Altmetric.com
Description
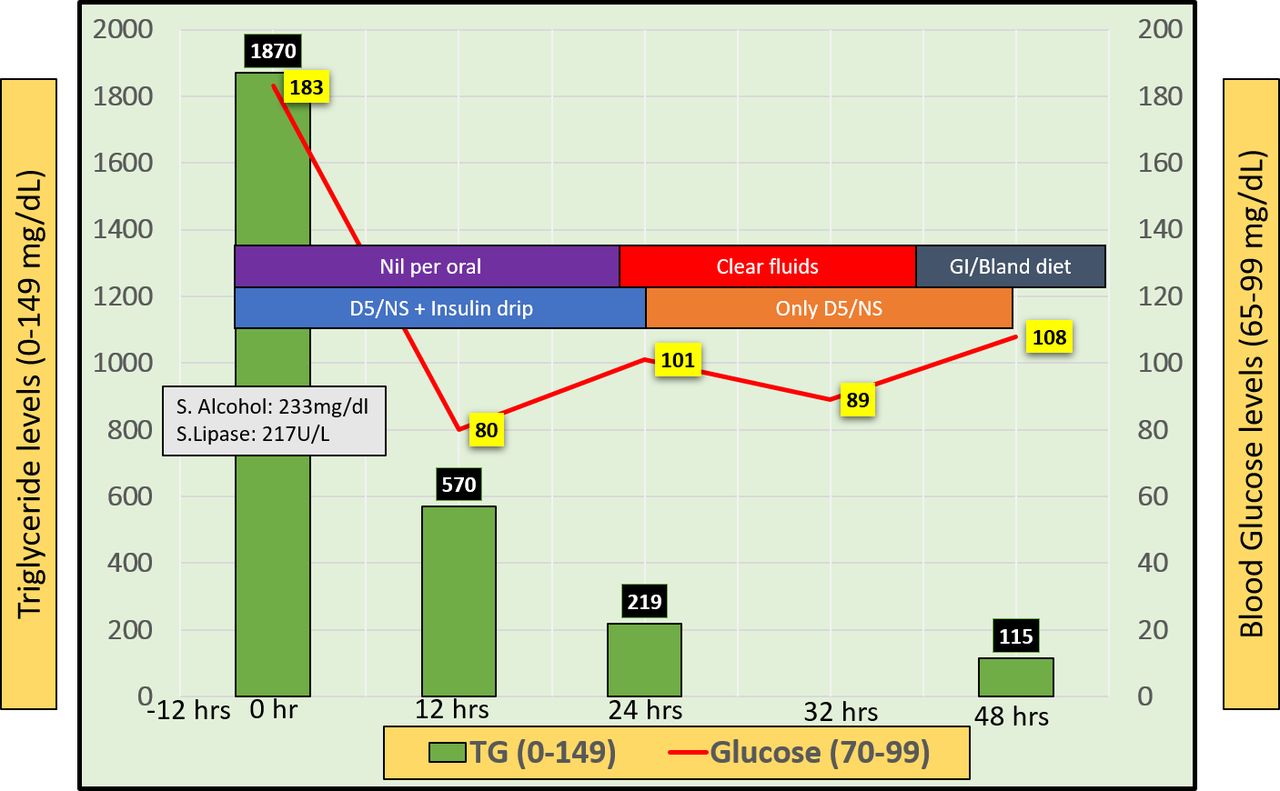
A 36-year-old woman came to emergency room for the complaint of acute onset pain in abdomen radiating to back l last 1 day. Medical history was significant for alcohol and substance use disorder with last binge alcohol drinking 12 hours prior to her emergency visit. Blood work suggested high blood alcohol levels (233 mg/dL), high lipase levels (450 U/L) and high triglyceride levels (1870 mg/dL). CT of abdomen showed severe and extensive peripancreatic inflammatory changes, surrounding the pancreas extending laterally towards both the paracolic gutters suggesting severe acute pancreatitis (figure 1). She was given 2 L of fluid bolus with normal saline and initiated on intravenous infusion of regular insulin 0.1 units/kg/hour, which was continued until next 24 hours until triglyceride level came down below 500 mg/dL (figure 2). Dextrose/normal saline was continued for next few days until patient started tolerating diet. Patient was prescribed oral gemfibrozil 600 mg twice daily and counselled for dietary modification and referred to detoxification centre to prevent further recurrence.
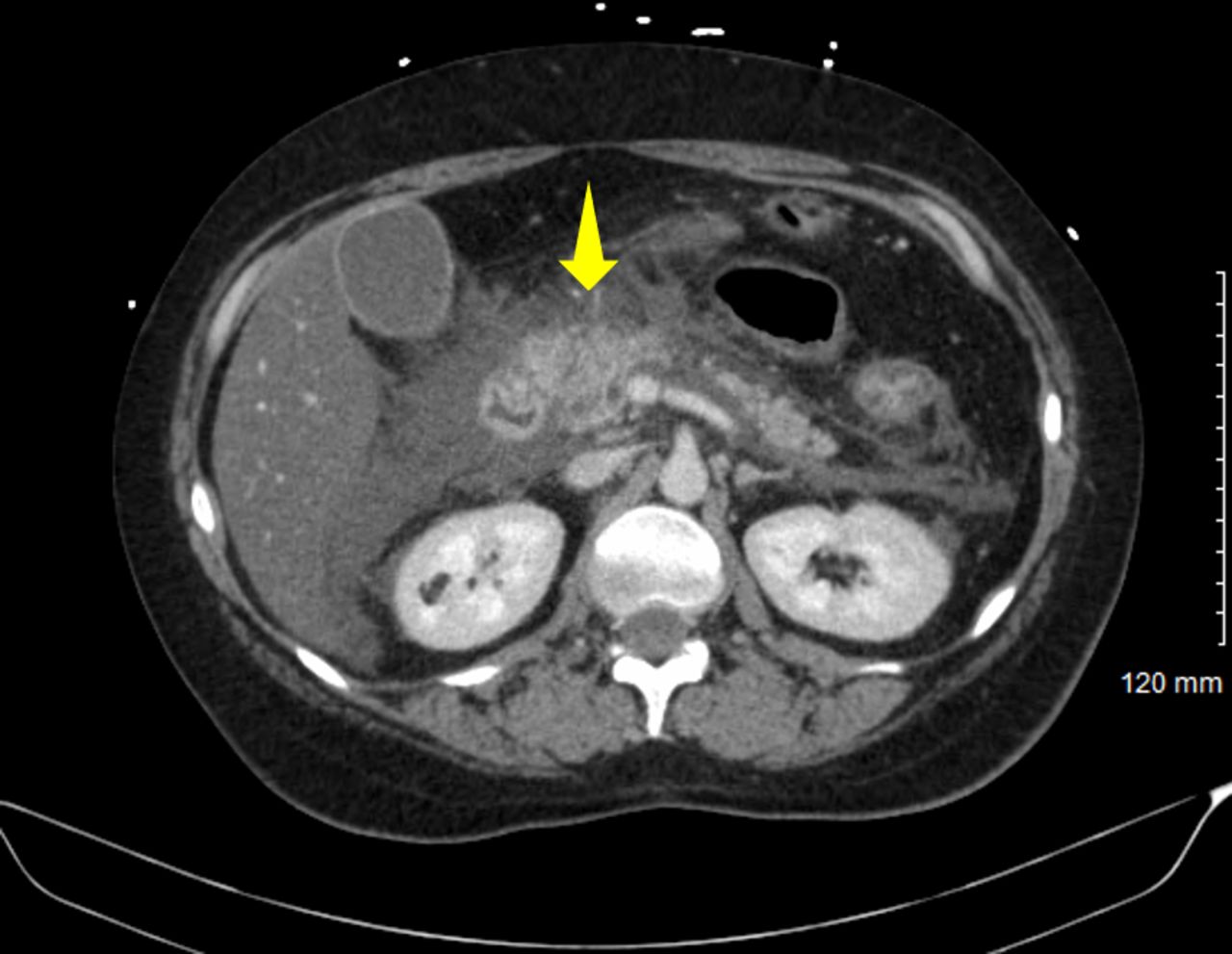
CT abdomen showing severe and extensive peripancreatic inflammatory changes, surrounding the pancreas extending laterally towards both the paracolic gutters.
{kind=link}
{kind=link}
Graph depicting the intensive care unit care during first 48 hours with timeline of using insulin drip, intravenous fluids and lab work results.
Like our case, Ramesh et al also reported successful outcome in a patient with hypertriglyceridemia induced acute pancreatitis.1 Imaging studies are very important in evaluating extremely rare and complicated abdominal diseases.2–4 While alcohol was a clear predisposition in our case, diabetes was likely the inciting factor in Ramesh’s et al case. which did not respond to insulin therapy and finally required two sessions of plasmapheresis. Recently, there has been debate about the use of plasmapheresis as an initial therapy versus in refractory cases. Cost, availability and complications are major concerns for considering plasmapheresis as an upfront modality of therapy. As per updates in the 7th edition of the American Society for Apheresis guidelines, plasmapheresis as an initial therapy can be considered in any one of the following: (1) hypocalcaemia; (2) lactic acidosis; (3) two or more signs of worsening inflammation; and (4) worsening organ dysfunction.5 To remember that, citrate anticoagulation during plasmapheresis has an independent survival benefit and hence recommended. Role of heparin is currently controversial as it is known to stimulate release of endothelial lipoprotein lipase, which promotes the conversion of triglycerides to free fatty acids, one of the lipotoxic agents, and hence heparin should not be used as an anticoagulation.6
A recent prospective RCT by He et al on 66 hypertriglyceridaemia-induced acute pancreatitis patients received either early high-volume haemofiltration (HVHF) or low molecular weight heparin (LMWH) +insulin as an emergent triglyceride-lowering therapy. As per the results, HVHF lowered triglyceride levels more quickly than LMWH+insulin therapy, but no difference was noted in terms of clinical outcomes, local pancreatic complications, need of surgery and costs.7 Apart from the indications, availability, benefits of early versus late, complications associated with use of plasmapheresis, cost is also an important factor that affects the choice of therapy. Plasmapheresis usually costs $250/session in developing countries compared with $1000 to $2000/session in developed countries.
Learning points
Hypertriglyceridemia induced acute pancreatitis is a rare and challenging entity and timely intervention is essential to prevent mortality.
Plasmapheresis is beneficial in rapid decrease of triglyceride levels without any survival benefit.
Footnotes
Contributors KKS: management and manuscript writing. AM: literature search and editing. AL: case review and write up. ES: critical comments and review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.