Article Text

Abstract
Fetus in fetu (FIF) is an extremely rare condition in which malformed fetus is found most commonly in the retroperitoneum of living twin. It occurs in about 1 in 500 000 live births and less than 200 cases have been reported in medical literature. We report FIF in a 17-year-old woman unlike other cases which were usually detected in early age and in male gender. This is the eighth case of adult FIF and the first case of FIF in adult woman worldwide. Preoperative diagnosis of FIF on CT was made and planned for exploratory laparotomy. The excised malformed fetus in a sac was proven as FIF on the basis of histopathological examination. In view to avoid such late presentation, early detection of FIF with radiological imaging in clinically suspected case is recommended. Surgical excision is the ideal treatment even teratoma is the differential diagnosis.
- congenital disorders
- pathology
- radiology
- general surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Fetus in fetu (FIF) is a rare developmental abnormality in which a malformed fetus is found within the body of other twin. It was first described by Johann Friedrich Meckel in the late 18th century. Majority of cases have been described in neonates and children and only seven cases have been reported after the age of 15 years (table 1). The first reported case of FIF in an adult man, whose age was 47 years, is by Dagradi et al 1 All reported cases of adult FIF were in male gender. We aim to report this case since to the best of our knowledge this case is the first case of FIF in a female gender of 17 years age and reviewing the literature.
Fetus in fetu in adult cases published in between 1999 and 2016
Case presentation
A 17-year-old woman presented with abdominal lump for 5 years, which was gradually increasing in size. It was associated with pain in abdomen which was on and off in nature. She was also complaining of early satiety but there was no history of significant weight loss. There was no history of altered bowel habits and urinary symptoms. Her menstrual history was within the normal limits. There was no history of twin birth or teratoma in the family. Her general, physical and systemic examinations were within the normal limits. On abdominal examination, there was a mass involving the whole of the abdomen (figure 1). This abdominal lump was firm to hard in consistency, its surface was irregular, margins were ill-defined and it was not moving with respiration. With these clinical information except to say abdominal tumour, it was not possible to conclude a final diagnosis.

Showing abdominal lump with ill-defined margin.
Investigations
On evaluation, beta-human chorionic gonadotropin (β-HCG), alpha feto protein and routine blood investigations were found within the normal limits. An abdominal contrast-enhanced computed tomography (CECT) scan showed a well-defined mass that measured approximately 25×23×15 cm, extending from epigastrium to upper pelvis (figure 2). It was showing fat density areas, soft tissue and multiple calcified density components of various sizes and shapes resembling the shape of vertebrae, ribs and long bones. This mass was causing displacement and compression of adjacent abdominal viscera.

Abdominal contrast-enhanced computed tomography showing 25×23×15 cm mass with multiple calcified densities compressing the adjacent abdominal viscera.
Differential diagnosis
On the basis of clinical findings (slow growing abdominal lump with firm to hard consistency, irregular surface and ill-defined margins) and CECT findings (well-defined mass with fat density areas and multiple calcified density resembling shape of vertebrae, ribs and long bones), a clinical diagnosis of FIF was made preoperatively.
Treatment
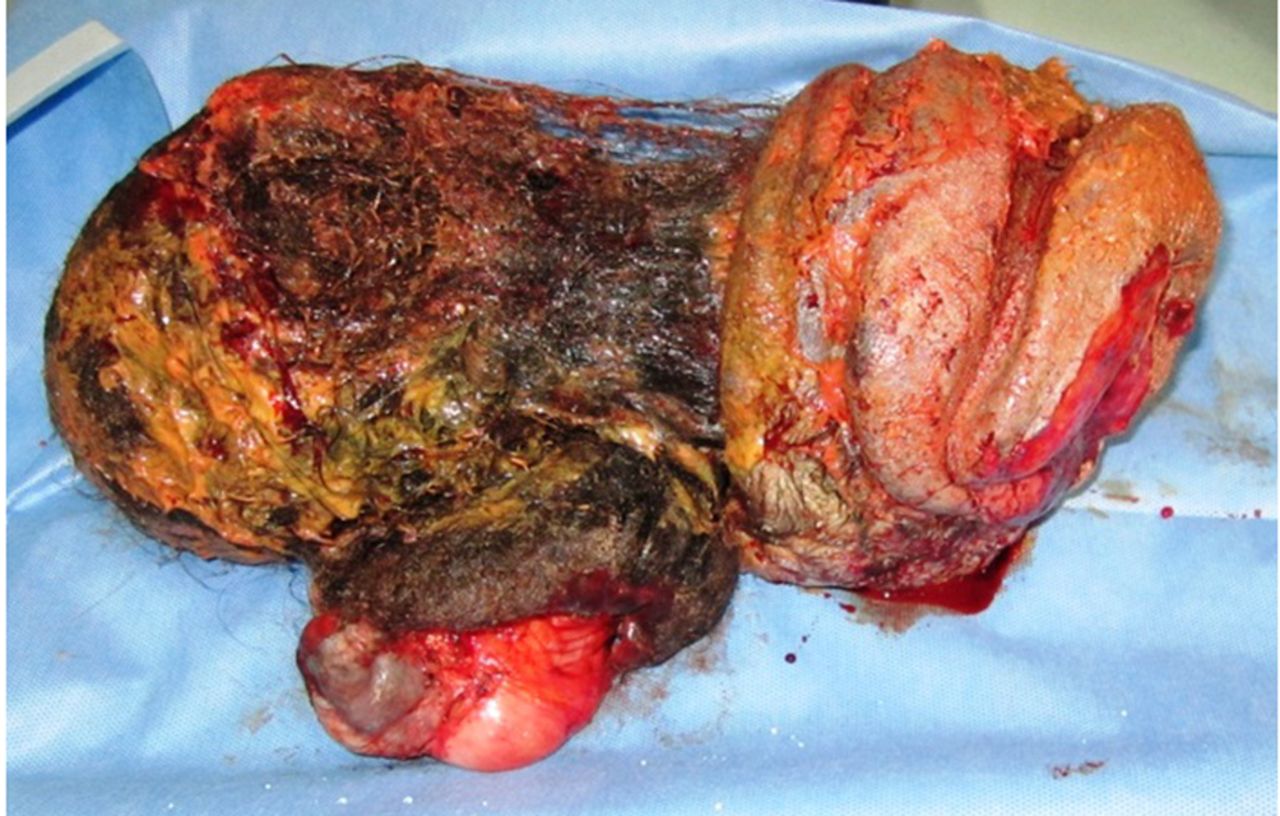
On exploration, there was a large retroperitoneal encapsulated mass, extending from the under surface of the liver reaching up to the pelvic rim (figure 3). It was grossly displacing intra-abdominal viscera however no invasion was noted. The contents of the tumour consisted of hairs, mature bones and other body parts (figure 4). The contents were removed in toto and a part of cyst wall which was densely adherent to the mesenteric vessels was left behind in order to prevent devascularization of gastrointestinal tract. The remaining cyst wall was cauterised. On macroscopic examination, the mass measured 30×16×10 cm and was composed of hairy cheesy material, multiple teeth and structures resembling limb buds. On cutting section, it showed fatty, cartilaginous and bony areas along with another cystic area of size 8×7 cm. Microscopically, there was an admixture of different elements including neural, intestinal, cartilaginous and bone along with skin adnexal structures and adipose tissue. However, no immature elements were seen. A final diagnosis of FIF was given on the basis of histopathological findings.

Showing encapsulated mass extending from the under surface of the liver reaching up to the pelvic rim.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Specimen consists of hairs, mature bones and other body parts.
Outcome and follow-up
Her postoperative period was uneventful. She has now been on our follow-up for the last 24 months with normal level of β-HCG and is doing well.
Discussion
FIF is a condition, commonly occurs in retroperitoneal space (80%).2 Others rare sites like sacrococcygeal region, intracranial, thorax, pelvis, scrotum, back and oral cavity have also been described in the literature.3–5 There are two theories for the development of FIF. One is parasitic twin theory in which parasitic malformed fetus formed inside the body of its host twin and share common blood supply. The parasitic twin is anencephalic with lack of many internal organs and it usually dies before birth.6 The other theory is that FIF is a highly differentiated form of teratoma.7 However, Willis (1953) emphasised the definition of FIF as a mass containing a vertebral axis along with other organs or limbs.8 Recently, many cases have reported as FIF without the presence of vertebral column but features of advanced stage of organogenesis.9
Majority of the reported cases of FIF are found in infancy and neonatal age group unlike our case.10–14 Excluding the present case, only seven adult cases of FIF have been reported in the literature.15 Among adult cases of FIF, the oldest and the youngest case was 47 years and 20 years old respectively, while the age of present case was only 17 years.1 16 In older age, although diagnosis is more in favour of retroperitoneal teratoma the possibility of FIF cannot be ruled out. Moreover it is in fact very difficult to differentiate these two conditions. Willis in 1953 set the criteria to differentiate these two conditions that FIF contains a vertebral axis with organs and limbs arranged around it, whereas teratoma is an accumulation of pluripotent cells in which there is neither organogenesis nor vertebral segmentation.17 The preoperative diagnosis of FIF can be made on radiological findings.18 Plain abdominal X-rays may be helpful in diagnosis of a vertebral column and axial skelton. A CECT would easily pick the presence of axial skelton and fatty tissue around it as in our case. Complete excision of FIF with its all surrounding membrane is the treatment of choice because of the possibility of malignant transformation.19 The possibility of malignant transformation is more found if the tissue of FIF remains left after surgery.20 Although the prognosis for FIF is more favourable than for cystic teratoma, the presence of immature elements mandates close clinical, radiological and serological follow-up to detect recurrence. This case will be follow-up at every year in view to detect malignancy as some adherent tissue was left during surgery.
Patient’s perspective
I was much worried about my abdominal lump, after operation I am feeling very well and my abdomen is now flat and my parents are also very happy. Thanks to all operating doctors.
Learning points
Fetus in fetu (FIF) is a rare condition usually occurs in infancy and child age group.
FIF in a 17-year-old woman is an extremely rare condition.
This case is the eighth case of adult FIF and the first case of FIF in adult woman worldwide.
Among all reported cases of adult FIF until, this case represents the largest size of FIF measured 36×16×10 cm.
References
Footnotes
Contributors Manuscript writing, editing and design: AK; concept and operating the patient: SSP; review of literature and radiological review of CT film: PK; review of the manuscript and literature search: BK.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.