Article Text

Abstract
Coronary artery aneurysm (CAA) is a rare cause of myocardial infarction. However, only a few studies have investigated this aspect. An 84-year-old woman with a history of hypertension presented with nausea. showed ST elevation in the inferior leads, and coronary angiography revealed two giant CAAs in the right coronary artery. Percutaneous coronary intervention was difficult because of risk of CAA rupture. Thus, these aneurysms were further evaluated using multimodality cardiac imaging to determine the treatment. MRI using late gadolinium enhancement revealed structural features of the aneurysms and the viability of the myocardium. Only antithrombotic medication was administered on the basis of the results of the multimodality cardiac imaging. Here, we report a rare case of a patient diagnosed with ST elevation myocardial infarction caused by thrombosis in giant CAAs using multimodality cardiac imaging, particularly MRI.
- ischaemic heart disease
- radiology (diagnostics)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Ischaemic heart disease is one of the most common causes of death, and its frequency is increasing worldwide. The mortality of patients with ST elevation myocardial infarction (STEMI) is influenced by many factors, such as advanced age, Killip class and delayed treatment.1–3 Guidelines for the management of STEMI emphasise that a patient with STEMI should be administered reperfusion therapy as soon as possible.1 4 Unfortunately, difficulty in performing primary percutaneous coronary intervention (PCI) sometimes delays time to reperfusion. A rare reason for this is the presence of Coronary artery aneurysm (CAA) in the culprit artery of infarction. However, because of the low incidence of CAA, it is detected only approximately 1.65% by coronary angiography (CAG). Moreover, studies on CAA are limited, and the treatment for patients with STEMI caused by CAA has not been established.5
Case presentation
An 84-year-old woman presented to her family doctor with nausea that persisted for 3 days. Her medical history included hypertension. There was no family history of cardiovascular disease. Because ECG showed ST elevation in the inferior leads, she was referred to our hospital with a diagnosis of STEMI. On arrival, she was asymptomatic. Vital signs and physical examination showed untoward features. ECG revealed ST elevation; thus, CAG was performed.
Investigations
On admission, blood examination revealed the levels of the following: creatine kinase, 285 IU/L and troponinT, 1.590 ng/mL. CAG revealed two giant CAAs in the right coronary artery (RCA) (figure 1). Distal end of these aneurysms was not defined; there was stenosis on the exit side of these aneurysms. PCI was difficult because of the risk of CAA rupture. Therefore, the following cardiac imaging examinations were performed to evaluate these aneurysms: transthoracic echocardiography, myocardial perfusion single photon emission computed tomography (SPECT), CT and MRI.

Coronary angiography revealing giant aneurysm (※) in right coronary artery.
Two large masses were observed near the aorta and in the right atrioventricular groove area by transthoracic echocardiography. Each mass was approximately 40×40 mm. Thrombosis was identified in the aneurysms.
Adenosine stress thallium-201 myocardial perfusion SPECT showed fixed defect in the inferior wall, and this result indicated myocardial infarction (MI) in the RCA territory.
Multidetector CT and volume rendering showed two giant CAAs followed by the RCA, and multiplanar reconstruction showed two giant CAAs and some thrombosis in one of the aneurysms (figure 2).

Multidetector-row CT. (A) Volume rendering imaging, (B) multiplaner reconstruction (→) show coronary artery aneurysms.
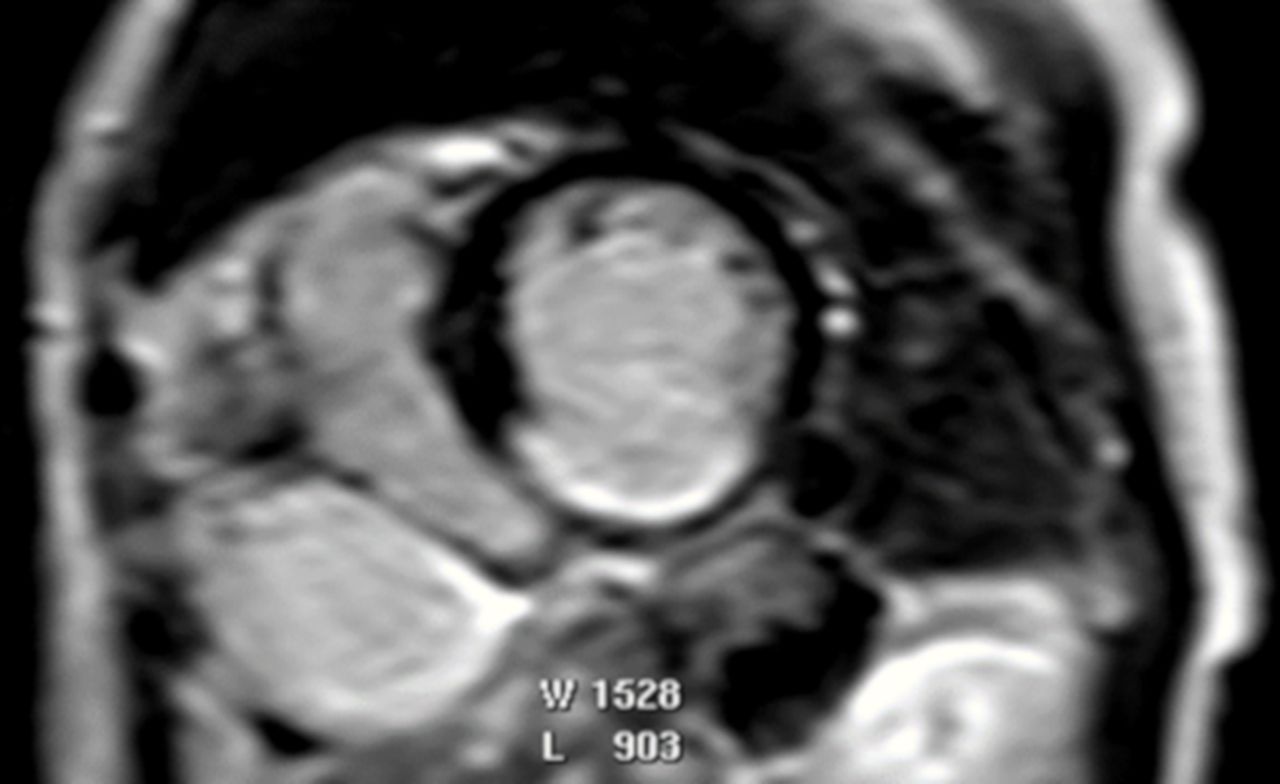
MRI revealed the shape of the CAAs and the viability of the myocardium (figure 3). Cine MRI revealed myocardial wall thinning and akinesis in the inferior wall, and late gadolinium enhancement revealed inferior myocardial scar with >50% transmurality. Cine MRI also showed turbulent flow in the CAA.

{kind=link}
{kind=link}
{kind=link}
MRI revealing wall thinning and late gadolinium enhancement in the inferior wall.
Therefore, these imaging modalities indicated that infarction of the inferior wall was caused by thromboses which were a consequence of turbulent flow in CAAs.
Treatment
Surgery was presented as a treatment option because of the risk of CAA rupture. Because she refused to undergo surgery, she was administered antiplatelet and anticoagulant agents: aspirin 100 mg/day and warfarin.
Outcome and follow-up
At 22 months from onset, she died of a sudden cardiac arrest. Her CT on autopsy showed massive pericardial effusion. The suggested direct cause of death was cardiac tamponade because of CAA rupture.
Discussion
In Japan, the peak age of female patients with acute myocardial infarction (AMI) is 80–89 years.2 Elderly individuals with MI exhibit various complications, with CAA being a rare complication. CAA is defined as local dilatations in the coronary that are 1.5-fold greater than normal adjacent segments.6 Because patients with CAA seldom have subjective symptoms, they are almost accidentally diagnosed. A study reported that the incidence of CAA was approximately 0.2%–2.6% diagnosed by CAG and was most common in the RCA.7 8 Moreover, approximately 50% of CAA are caused by atherosclerosis, followed by congenital disease (20%–30%). Kawasaki disease, autoimmune disorder and injury also cause CAA.9 However, the specific mechanisms that drive the formation of CAA remain unclear because of its rarity.6
The treatment for patients with STEMI caused by CAA has not been established. A previous study reported that MI was caused by CAA in an elderly patient who underwent PCI by covered stent implantation.10 In contrast, Yanik et al said that a conservative approach is recommended in asymptomatic patients with MI because it is difficult to cross the thrombosed outlet of the CAA and there is a risk of rupture by intervention wire.11 In addition, a few studies have reported that anticoagulation therapy reduces the risk of MI and sudden cardiac arrest in patients with CAA.12 13 Furthermore, another study recommends surgical treatment for all CAAs that are >3 cm because of the risk of rupture.14
Generally, CAA is diagnosed by transthoracic echocardiography, CAG and CT. A few reports have mentioned the use of MRI for diagnosing CAA.15 16 Particularly, cine MRI can be used to image cardiac motion, including CAA, turbulence of blood flow and myocardial asynergy by aneurysm. Late gadolinium enhancement MRI (LGE-MRI) is also useful for determining invasion depth of subendocardial infarction. Choi et al reported the diagnostic capabilities of LGE-MRI in patients with AMI who had an onset within 1 week.17 Kitagawa reported the transmural extent of infarcted myocardium, and >50% had evaluated the absence of myocardium viability.18
In the presented case, PCI was difficult because of the risk of CAA rupture by intervention wire, and she was asymptomatic during CAG. Multimodality images revealed that the thrombosis in CAAs has resulted in coronary artery stenosis. Furthermore, LGE revealed inferior myocardial scar with >50% transmurality. Surgery was recommended due to the risk of CAA rupture; however, the patient refused to undergo surgery. Hence, she was administered medication. Consequently, she survived for only 22 months from onset. Transthoracic echocardiography, CT and MRI were used for determining the condition of CAA. In this case, multimodality imaging, including MRI, contributed in making the treatment decision. Moreover, MRI is a non-invasive modality without the risk of radiation exposure and can help in determining the characteristics of the myocardium and anatomical cardiovascular structures.
In conclusion, multimodality imaging, including MRI, are useful in the diagnosis of MI caused by CAA. Further studies on CAA are essential to decrease mortality by CAA and establish the guidelines for treatment.
Learning points
Treatment of coronary aneurysm is different in each case and depends on size of the aneurysm or condition of patients.
This is a rare case of a patient diagnosed with ST elevation myocardial infarction caused by thrombosis in giant coronary aneurysms using multimodality cardiac imaging, particularly MRI.
Knowing the shape of the coronary aneurysms and the condition of the myocardium using various imaging techniques can help in determining the best treatment, considering the background of patients.
References
Footnotes
Contributors SH and YS designed the manuscript, and wrote the initial draft. SH, YS and TY contributed to analysis and interpretation of data. YS and TY assisted in the preparation of the manuscript. ET have contributed to data collection and interpretation, and critically reviewed the manuscript. All authors approved the final version of the manuscript, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Next of kin consent obtained.