Article Text

Abstract
Orthostatic headache (OH) is a key symptom of spontaneous intracranial hypotension (SIH). However, there is no optimal history taking for OH. A 35-year-old man complained of headache that prevented him from performing routine physical activities, which was relieved on lying down. We initially considered migraine as the most likely diagnosis. However, detailed history taking revealed that his headache worsened on standing, and he was finally diagnosed with SIH. Headache relief on lying down is not a specific indicator of OH associated with SIH. Thus, with regard to headache history taking, we suggest it important to confirm headache aggravation on standing.
- headache (including migraines)
- neuroimaging
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Spontaneous intracranial hypotension (SIH) is a rare cause of headache. However, it should be considered in the differential diagnosis of cases of new daily persistent headache because a good outcome can be achieved with appropriate treatments, such as bed rest and epidural self-blood patch therapy.1 Although orthostatic headache (OH) is not included in the SIH diagnostic criteria of the International Classification of Headache Disorders 3rd edition (ICHD-3), it is a useful indicator of SIH because other symptoms, such as nausea and tinnitus, are non-specific.2 Thus, it is important to take a proper history of this headache for the diagnosis of SIH.
We herein report the case of a patient with SIH who had a delayed diagnosis because we did not identify the patient’s feeling of headache relief on lying down as OH.
Case presentation
A 35-year-old man presented to our hospital with worsening of his headache pattern over the last 38 days. He had intermittent and non-pulsatile headache with nausea on every day. The duration of his headache was about 4–8 hours. He had a medical history of migraine since around the age of 20 years and experienced his first headache at 15 years of age. Therefore, he could not state whether the present headache was similar to the previous headaches. He denied any recent history of head trauma. On physical examination, no remarkable findings were noted, including vital signs and neurology findings.
Initially, we suspected a relapse of migraine because he complained that he could not work owing to headache with nausea and that the headache was relieved by lying down. Non-steroidal anti-inflammatory drugs and triptan were prescribed, but they were ineffective. Forty-two days after onset, he was referred to an otorhinolaryngologist at another hospital for his complaint of tinnitus and was found to have mild sensorineural hearing loss on both sides. Because his headache worsened further, he was admitted to our hospital 54 days after onset.
On admission, detailed medical history revealed that his headache reduced 30 min after resting on a bed and worsened within 10 min of standing.
Investigations
CT showed chronic subdural haematomas (CSHs) on both sides, and gadolinium-enhanced MRI showed an enhancement of the pachymeninges, engorgement of venous structures and ventricular collapse (figure 1). Based on these findings, we diagnosed SIH with bilateral CSHs.
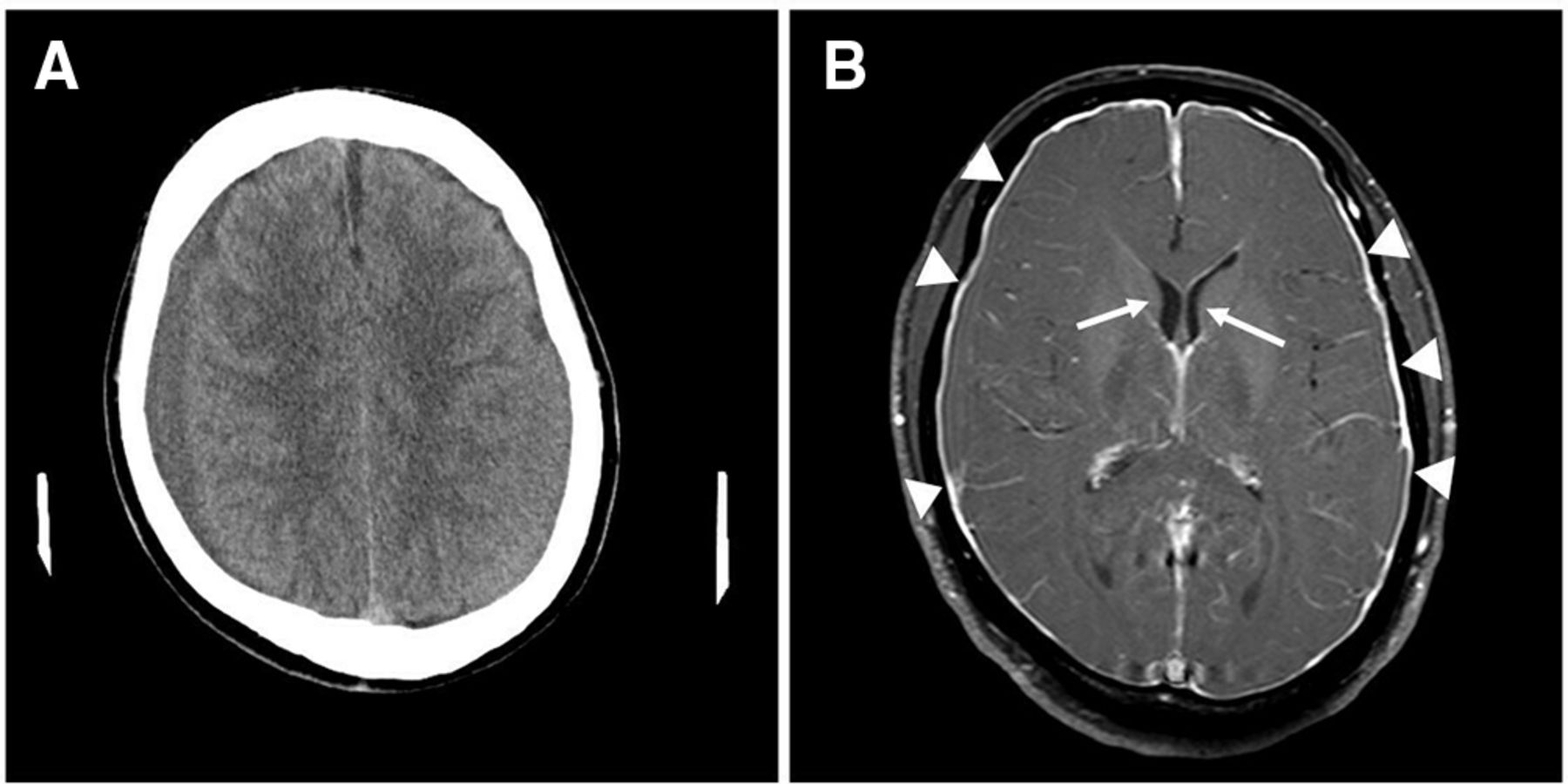
(A) Head CT on day 54 after onset showing chronic subdural haematomas on both sides. (B) Gadolinium-enhanced MRI on the same day showing findings of spontaneous intracranial hypotension, including an enhancement of the pachymeninges (arrowheads) and ventricular collapse (arrows).
Treatment
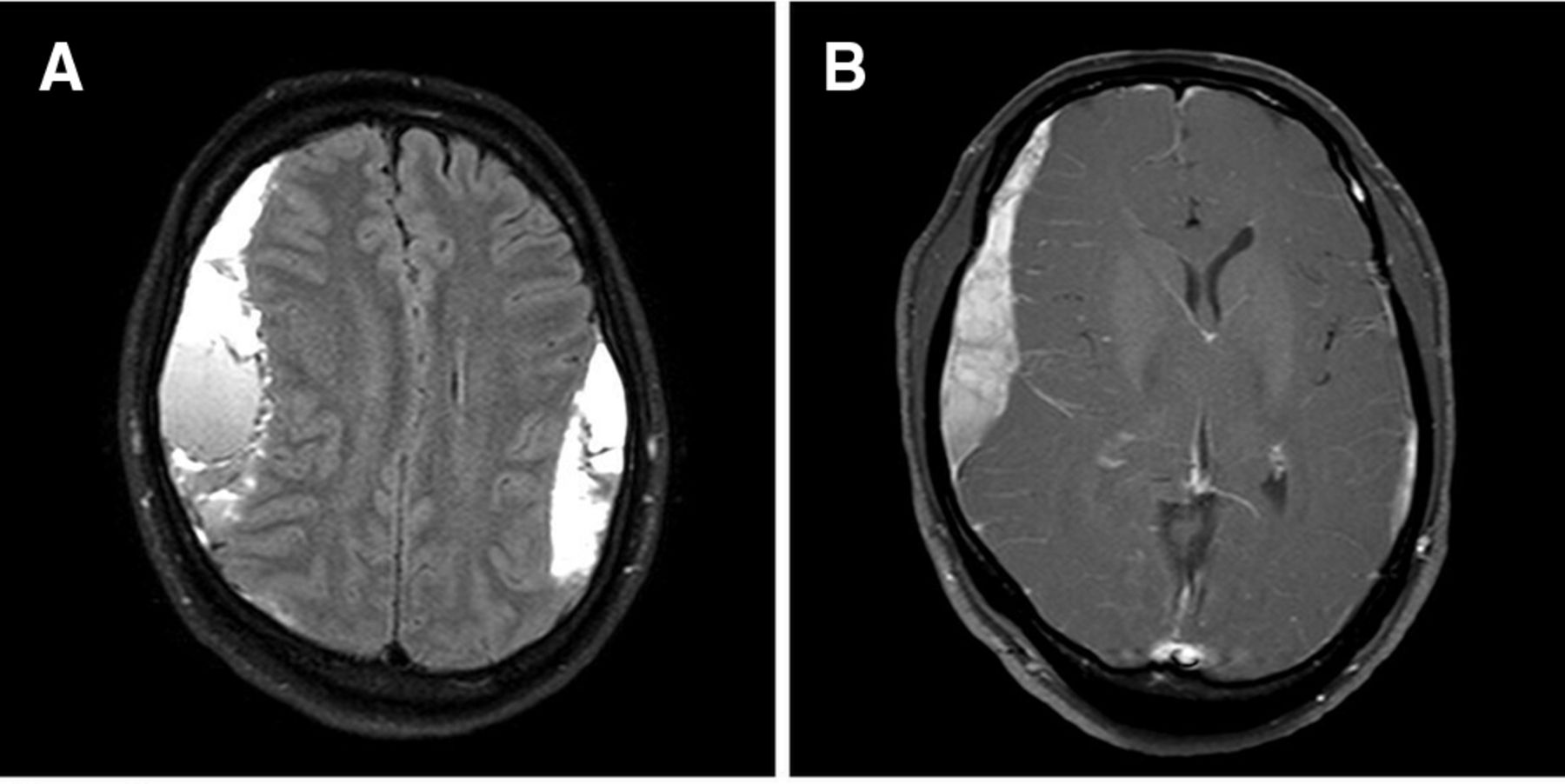
After admission, we instructed him to take bed rest in the recumbent position and carefully monitored his neurological symptoms and imaging findings. His headache temporarily worsened and haematoma increased (figure 2), but his condition gradually improved, and he was discharged on day 69 after admission (day 124 after onset).

{kind=link}
{kind=link}
MRI on day 79 after onset. (A) Fluid-attenuated inversion recovery showing increasing chronic subdural haematomas on both sides. (B) T1-weighted views after intravenous administration of gadolinium showing a decreased enhancement of the pachymeninges.
Outcome and follow-up
He returned to work without any symptoms 1 month after discharge, and MRI on day 219 after onset revealed that the CSHs almost disappeared.
Discussion
Headache associated with SIH is caused by spontaneous spinal cerebrospinal fluid (CSF) leakage.2 The cause of CSF leakage remains largely unknown, but an underlying structural weakness of the spinal meninges, which is associated with connective tissue disorders such as Marfan syndrome, has been suspected.1 However, our patient did not have any finding of such diseases. Previous reports have reported cases associated with minor trauma or exercise.3–6
In many cases of SIH, a conservative approach such as bed rest and oral hydration is effective and in severe case, the injection of autologous blood into the spinal epidural space (epidural blood patch) is the mainstay treatment.1 In a severe case of CSH, surgical therapy is recommended. However, in case of SIH with CSH, the optimal treatment is controversial.7 In this case, we first tried conservative treatment for SIH and haematoma increased. Because his symptoms gradually improved, we continued conservative therapy. As a result, he got a better without epidural blood patch and surgery.
Epidemiology data regarding SIH are limited, but Schievink has reported its peak incidence at around 40 years of age.1 MRI is important for diagnosis of SIH. The five characteristic MRI features of SIH include (1) subdural fluid collection, (2) enhancement of the pachymeninges, (3) engorgement of venous structures, (4) pituitary hyperemia and (5) sagging of the brain.1 Subdural fluid collection is observed in ~50% of SIH cases8 and enhancement of the pachymeninges in 83%.3
ICHD-3 has presented the following SIH diagnostic criteria: (A) headache fulfilling criterion C below, (B) absence of a procedure or trauma known to be able to cause CSF leakage, (C) headache has developed in temporal relation to occurrence of low CSF pressure or CSF leakage, or has led to its discovery, and (D) not better accounted for by another ICHD-3 diagnosis.2 Previously, SIH diagnostic criteria (ICHD-2) included OH, which is diffuse and/or dull headache that worsens within 15 min after sitting or standing.9 But in some patients, this lag period may be prolonged to several hours. Therefore, ICHD-3 describes the usefulness of OH but its diagnostic criteria do not include it. Chung et al reported that almost all SIH patients have OH and that other symptoms include nausea (53%), dizziness (30%), neck stiffness (17%), plugged ear (20%) and tinnitus (20%).3 Because these symptoms are non-specific, patients with SIH are commonly misdiagnosed, which results in a diagnostic delay.10 Therefore, it is important to take a proper history of OH.
In the present case, at the initial history taking, the patient mentioned that he could not work owing to headache and that the headache was relieved by lying down. We recognised it as a characteristic of migraine that is aggravated on activity and causes an avoidance of routine physical activity and thus, misdiagnosed the patient with migraine. After 2 weeks, further history taking indicated OH because his headache recurred within 10 min after rising from the recumbent position.
On taking medical history, OH is suspected if a patient’s headache is relieved on lying down and aggravated on standing. However, in several diseases, patients experience headache relief on lying down. Therefore, only headache relief on lying down may indicate common causes of headache, such as migraine and tension, rather than SIH.
Because OH associated with SIH may show a delayed response to postural change, with worsening after minutes or hours on standing and improvement after minutes or hours on lying down,2 3 an optimal history taking of OH has not been reported. In the present case, if headache aggravation on standing would have been identified at the initial assessment, then the condition may have been diagnosed earlier.
We herein reported a patient with SIH who had a delayed diagnosis because we did not identify the patient’s feeling of headache relief on lying down as OH. With regard to headache history taking for the diagnosis of SIH, we suggest that it is important to confirm not only headache relief on lying down but also headache aggravation on standing.
Learning points
Headache which is new onset and aggravation is suggested secondary headache.
Headache relief on lying down is not specific to spontaneous intracranial hypotension.
In history taking of orthostatic headache, it is important to confirm headache aggravation on standing.
Acknowledgments
JI, the corresponding author, is the patient in the presented case. He would like to thank Dr T Kawabe who is the neurosurgeon of Kyoto Prefectural University of Medicine. He also thank all Neurosurgical ward staff of University Hospital, Kyoto Prefectural University of Medicine.
Footnotes
Contributors JI designed the study and wrote the initial draft of the manuscript. KS critically reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.