Article Text

Abstract
A 78-year-old woman visited the emergency department with complaints of progressively worsening abdominal pain for a week. Nausea and vomiting started at the time of the visit. An abdominal contrast-enhanced CT (CECT) revealed a filling defect of portal vein, splenic vein and superior mesenteric vein (SMV) which was diagnosed as portal vein and mesenteric venous thrombosis (MVT). Intravenous administration of unfractionated heparin was initiated. However, her symptoms did not improve, and she underwent surgical thrombectomy on the second day of hospitalisation. On the sixth day, CECT revealed the recurrence of thrombi in the portal vein, SMV and along the central venous catheters. We switched heparin to argatroban on the eighth day. After administering argatroban, CECT revealed that the thrombi had almost disappeared by the 40th day. In this case, argatroban was considered effective for heparin-resistant and surgery-resistant portal vein and MVT.
- venous thromboembolism
- stomach and duodenum
- haematology (incl blood transfusion)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Mesenteric venous thrombosis (MVT) is a relatively rare but fatal disease. If conventional treatment modalities such as intravenous administration of heparin and surgical thrombectomy are ineffective, there are no established alternative treatment options.
Case presentation
A 78-year-old woman visited the emergency department with complaints of progressively worsening abdominal pain for a week. She began to feel nausea and to vomit at the visit. Her medical history included hypertension, dyslipidaemia and type 2 diabetes mellitus. At the time of presentation to the emergency department, her vital signs were as follows: blood pressure, 145/71 mm Hg; pulse rate, 90/min; respiratory rate, 24/min; oxygen saturation, 95% on room air and body temperature, 35.8°C. Her height was 142.0 cm; weight was 64.4 kg and her body mass index was 31.9 kg/m2. On physical examination, her abdomen was distended and bowel sounds were hypoactive. In addition, she had generalised abdominal tenderness with guarding.
Investigations
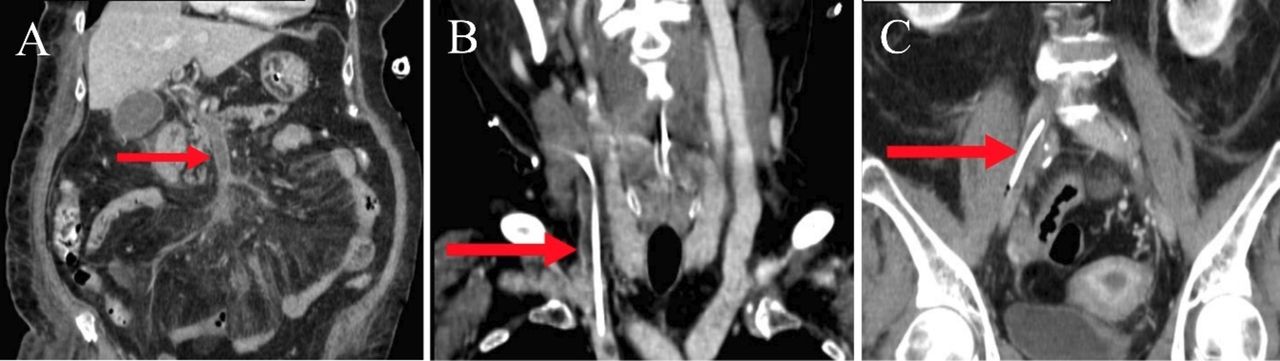
The results of the haematological, biochemical and coagulation investigations were as follows: platelet count, 157×109/L; haemoglobin, 133 g/L; haematocrit, 40.2%; white blood cell count, 17.9×109/L; C reactive protein level, 16.44 mg/dL; lactate dehydrogenase level, 267 IU/L; D-dimer level, 48.0 µg/mL (0–5.0 µg/mL); fibrin/fibrinogen degradation products (FDP) level, 94.8 µg/mL (0–10 µg/mL); fibrinogen level, 438 mg/dL (170–410 mg/dL); protein S, 127% (60%–127%); protein C, 111% (64%–135%); antithrombin III, 120% (80%–130%); anticardiolipin antibodies, negative and antiphospholipid antibodies, negative. An abdominal CECT revealed a filling defect of the portal vein, the splenic vein and the superior mesenteric vein in addition to thickening of the jejunal wall (figure 1).

Contrast-enhanced CT on admission showed a defect in the portal vein (A, C; arrow) extending to the superior mesenteric vein (B; arrow), in which thrombus was suspected, in addition to thickening of the jejunal wall (C; arrow).
Differential diagnosis
Portal vein and superior mesenteric vein (SMV) thrombosis.
Associated neoplasm (with extrahepatic venous thrombosis).
Superior mesenteric artery thrombosis.
Intestinal obstruction.
Gastroenteritis.
Congenital disease with antithrombin deficiency.
Disseminated intravascular coagulation.
Thrombotic microangiopathy.
Treatment
On the basis of the diagnosis, we administered intravenous unfractionated heparin of 15 000 IU/day as the initial treatment. However, owing to gradual worsening of the patient’s general condition and abdominal symptoms, emergent thrombectomy was performed as intestinal necrosis was suspected on the second day. As a result, she did not require any bowel resection. After the operation, we initiated intravenous administration of urokinase at 240 000 IU/day and unfractionated heparin at 15 000 IU/day. However, on the sixth day of hospitalisation, CECT revealed the recurrence of thrombi in the portal vein, SMV and along the central venous catheters (figure 2). The haematological and coagulation examination revealed reduced platelet count and an accelerated fibrinolytic system (platelet count, 65×109/L; FDP, 314 µg/mL; D-dimer, 177.7 µg/mL; fibrinogen level, 100 mg/dL; prothrombin time international normalized ratio, 1.29). On the eighth day of hospitalisation, the platelet count decreased to 23×109/L. Intravenous argatroban administration at a dose rate of 2.0 µg/kg/min was initiated because heparin-induced thrombocytopenia (HIT) type 2 was suspected; however, HIT antibody (PF4-H) was negative.
{kind=link}
{kind=link}
CECT on the eighth day of hospitalisation showed that thrombi were found in the inferior vena cava (A, arrow), the right internal jugular vein (B, arrow) and the right iliac vein (C, arrow) along the central venous catheter.
Outcome and follow-up
On the 11th day of hospitalisation, the platelet count had improved (68×109/L). On the 21st day of hospitalisation, intravenous administration of argatroban was changed to oral administration of edoxaban (60 mg/day). The platelet count had increased to 188×109/L on the 20th day of hospitalisation. Most of the thrombi had disappeared by the 40th day of hospitalisation. The remainder of her hospital stay was uneventful, and she was discharged on the 42nd day of hospitalisation. She was prescribed edoxaban (60 mg/day) and followed up every month. Five months after discharge, the dose of edoxaban was changed to 30 mg/day. She has had no recurrent venous thrombosis for 10 months after discharge.
Discussion
MVT is a relatively infrequent disease. The proportion of SMV thrombosis is reported to be 1 out of 5000 to 15 000 hospitalised patients, and 1 out of 1000 patients in emergency outpatient department. Six to nine per cent of patients with acute mesenteric ischaemia were found to have MVT.1 MVT has a varying clinical course from acute onset to chronic disease. The chief complaint of the patient is often abdominal pain. Therefore, when a patient with high thrombotic risk (eg, thrombophilia such as protein C or S deficiency, malignancy, myeloproliferative disorder, JAK2 gene mutation, liver cirrhosis and nephrotic syndrome) is admitted with a complaint of abdominal pain, MVT should be suspected and CECT or magnetic resonance angiography should be performed.2 In this case, according to the results of various examinations except the examination of JAK2 gene mutation, the patient did not have thrombotic risk factors such as those mentioned above. We clinically diagnosed idiopathic MVT because we were unable to determine the underlying aetiology.
We started 15 000 IU/day of heparin to maintain activated partial thromboplastin time level within 2–2.5 times the normal range, in reference to Liu et al.3
However, due to the gradual worsening of the patient’s general condition and abdominal symptoms, emergent thrombectomy was performed as intestinal necrosis was suspected.1 4 5 After the diagnosis of MVT, if intestinal perforation, intestinal necrosis and peritonitis are suspected, operation therapy should be selected.1 On the other hand, interventional radiological options, such as endovascular mechanical thrombectomy and catheter-directed thrombolysis, can be considered in patients at risk for bowel infarction but without peritonitis.1 Even after the operation, thrombi rapidly recurred. We considered that there was a hypercoagulable state with the same cause as the unclear mechanism is associated with the first MVT and that this state caused the recurrent thrombi and thrombocytopenia after surgery. We also suspected HIT because of the use of heparin and the recurrent thrombosis and thrombocytopenia. To resolve this clinical problem a latex agglutination examination for the PF4-H was conducted, and we changed the treatment for HIT from intravenous administration of unfractionated heparin to intravenous administration of argatroban which is a direct thrombin inhibitor.4 5 The PF4-H test result subsequently became negative. However, fortunately, argatroban was so effective that both thrombosis and thrombocytopenia improved.
Argatroban has an inhibitory effect on the conversion of fibrinogen to fibrin and also activates antithrombin function and fibrinolytic action.6 7 Furthermore, it has been reported that the mortality rate of patients who promptly received argatroban after diagnosis was 0%, which is as good as the mortality rate reported previously (0%–38.5%) using conventional anticoagulation therapy.8 Therefore, intravenous argatroban was found to be effective in the treatment of heparin-resistant and surgery-resistant MVT.
Learning points
When a patient with high thrombotic risk is admitted with a complaint of abdominal pain, mesenteric venous thrombosis (MVT) should be suspected.
Contrast-enhanced CT is a good diagnostic choice to confirm MVT.
Physicians should repeatedly evaluate the general condition and abdominal findings of patients with MVT who are treated with an anticoagulant because some patients require surgical treatment.
Argatroban may be considered in patients who have both heparin-resistant and surgery-resistant MVT.
Footnotes
Contributors TY: planning, concept and writing. YY: planning, data collection and writing. MS and KS: final corrections, proof reading and interpretation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.