Article Text

Statistics from Altmetric.com
Description
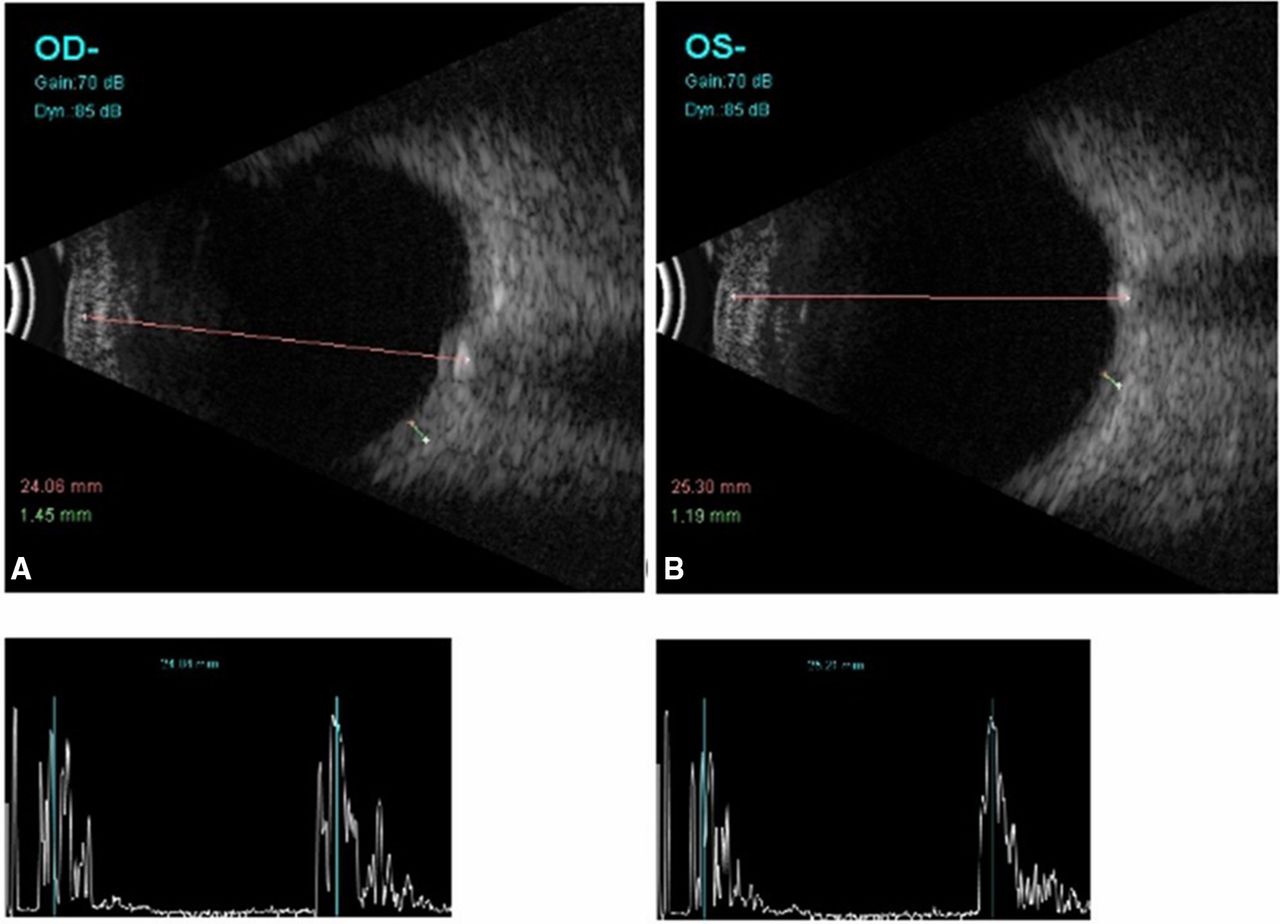
A 17-year-old boy presented with sudden painless diminution of vision in right eye for 3 days. The best corrected visual acuity was 20/400 and 20/20 in right and left eye, respectively. The intraocular pressures were 12 mm Hg in both eyes. There was associated relative afferent pupillary defect in right eye (OD). Anterior segment examination was otherwise normal in both eyes (OU). Dilated fundus examination OD revealed optic disc oedema with hyperaemia, extensive intraretinal haemorrhages, engorged tortuous veins, macular oedema and cotton wool spots (figure 1A). Left eye had a swollen disc with blurred margins and the physiological cup was obscured(figure 1B). Optical coherence tomography (OCT) through macula in right eye showed thickened retinal nerve fibre layer, intra-retinal cystoid spaces and neurosensory detachment (figure 2A). B-scan ultrasound revealed pronounced disc oedema OD and an ovoid echogenic lesion deep within the optic disc with corresponding high amplitude spike on A-scan OU (figure 3A,B). He did not report any medical history and was not on any systemic medications. Based on above clinical and imaging findings, a diagnosis of optic disc drusen OU and central retinal vein occlusion (CRVO) with macular oedema OD was made. Investigations for thromboembolic risk factors were unremarkable. His blood pressure (120/80 mm Hg), fasting blood glucose (86 mg/dL) and serum lipid profile were normal. The macular oedema ebbed with two intravitreal bevacizumab (1.25 mg) injections at 1 month intervals and the corrected vision improved to 20/80 at 3 months before he was lost to follow-up (figure 2B).
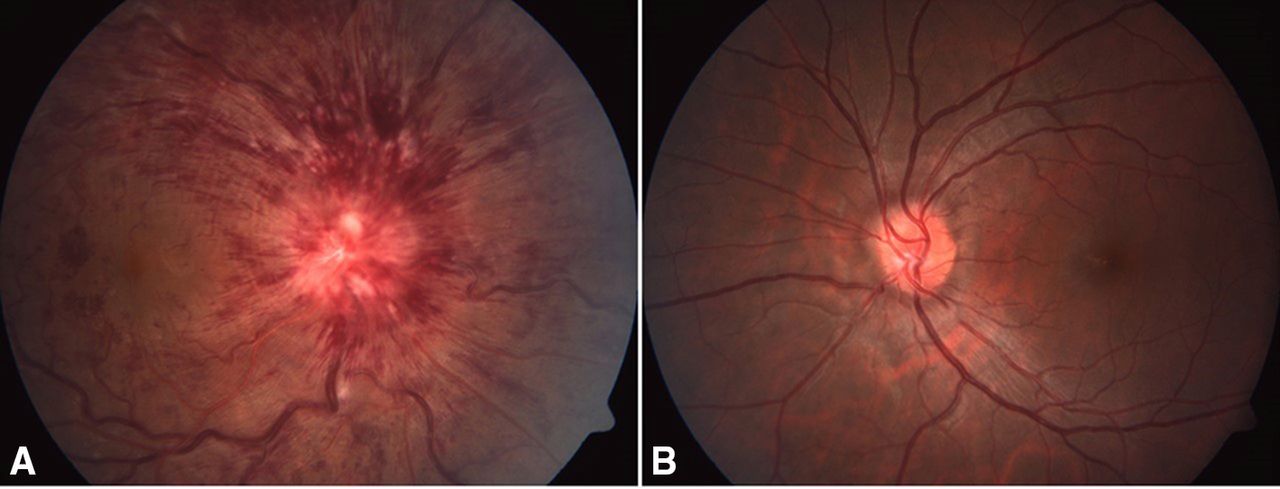
Colour fundus photograph of right eye (A) shows hyperemic and swollen disc with extensive intraretinal and disc haemorrhages suggestive of CRVO. Similar optic disc features sans the retinal haemorrhages in left eye (B) is suggestive of pseudopapilloedema. CRVO, central retinal vein occlusion.

Horizontal optical coherence tomography scan through macula in right eye (A) shows cystoid oedema of outer nuclear and plexiform layer, neurosensory detachment and thickening of retinal nerve fibre layer. A marked reduction in oedema is noted after treatment with intravitreal bevacizumab (B).
{kind=link}
{kind=link}
{kind=link}
Ultrasound B-scan image shows high reflective ovoid lesion at the optic disc representative of optic disc drusen in both eyes. OD,right eye; OU, both eyes.
Optic disc drusen are calcified hyaline-like deposits in the optic nerve head concentrated anterior to the lamina cribrosa.1 It’s incidence is 0.4%–20.4% in general population with female preponderance.2 They are often bilateral (67%–91%) and are commonly found at the nasal aspect of the optic disc.2 Largely they are benign and vision sparing but rarely may complicate with visual field defects, haemorrhages, choroidal neovascularisation, serous maculopathy and non-arteritic ischaemic optic neuropathy.3–5 Enlargement of drusen with advancing age is believed to cause mechanical compression at the lamina cribrosa leading to the complications.1 Elevation of central retinal venous pressure may result in CRVO.1 2 6 The enlargement is observed mostly in teenage7 8 but to the best of our knowledge only a single case has been reported with concomitant CRVO in teenage.9 Unlike the hitherto reported case which resulted in neovascular glaucoma and retinal detachment, we achieved favourable outcome with intravitreal bevacizumab injection in the early treatment period. Follow-up at a later date could throw light on the long-term course of this vascular occlusion. This underscores active and early treatment of symptomatic CRVO in young when associated with optic disc drusen. Universal eye screening in children could go a long way detecting optic disc drusen early and imaging modalities such as ultrasound B scan and enhanced depth optical coherence tomography can increase the sensitivity of the detection in buried drusen.10 11 Table 1 lists the reported association of optic disc drusen with CRVO in literature.
Patient demographics of the reported cases of CRVO association in eyes with optic disc drusen
Patient’s perspective
I am happy that my disease could be diagnosed accurately at an early stage and the treatment in the form of eye injection restored my vision. I was informed about the rarity of the haemorrhagic complication and the risk of the other eye being involved.
Learning points
Subjects with optic disc drusen should be made aware of the ominous prospects of a venous occlusion and followed closely.
Ultrasound B scan of optic nerve head is a simple imaging tool to reveal embedded drusen.
Optic disc drusen should be one of the differentials in young onset central retinal vein occlusions.
Acknowledgments
Hyderabad Eye Research Foundation.
Footnotes
Contributors SKP was involved in conceptualisation, data collection, manuscript writing and critically reviewing the manuscript. UCB was involved in planning, conceiving and conducting the study. He also wrote and critically reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.