Article Text

Statistics from Altmetric.com
Description
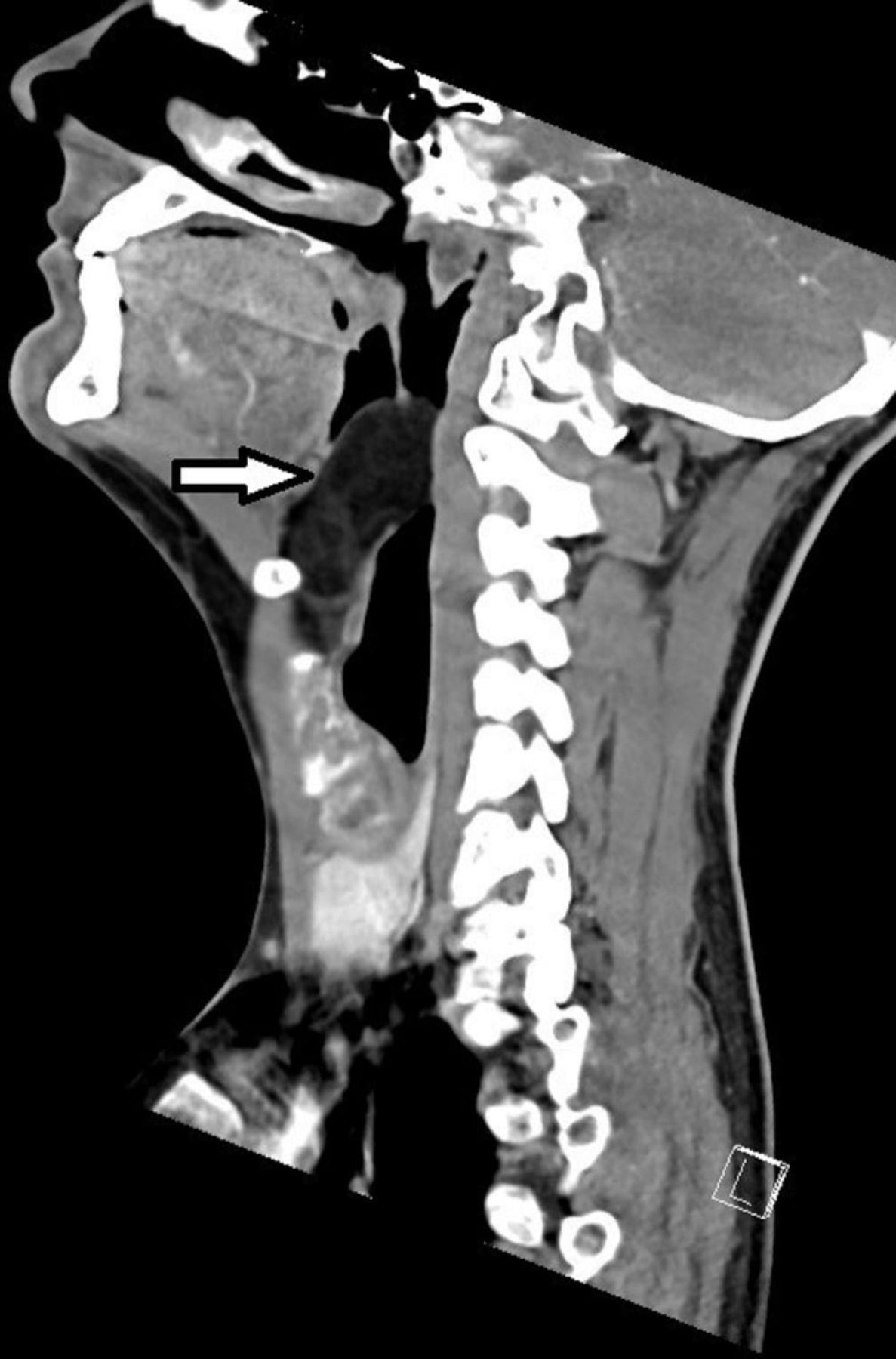
A 28-year-old man presented to the ear, nose and throat outpatients clinic with a 5 year history of voice change and a 1 year history of dysphagia and worsening shortness of breath on lying prone. His partner had noted recent noisy breathing at night. He was systemically well with no past medical history of note and smoked 5 cigarettes/week. On examination he had a ‘hot potato’ voice. Flexible nasendoscopy revealed a large right-sided mass that appeared to arise from the vallecula and occupied most of the oropharynx, with only the posterior glottis visible. CT imaging revealed a 56×38×26 mm lesion occupying the right vallecula causing significant airway obstruction (figure 1). Its contents were consistent with a fatty lesion. The following day he underwent awake fibreoptic intubation, debulking of the lesion orally followed by laryngoscopy and endoscopic excision. Histology confirmed a submucosal benign lipoma.

Sagittal CT of the neck shows lipoma in the vallecula (arrow).
Lipomas are rarely found in the upper aerodigestive tract, making up only 1–4% of all benign tumours of the oropharynx and oral cavity.1 These tumours are typically slow growing. However, they have the potential to cause airway obstruction depending on size and location and have been reported to cause stridor and death.2 3
Oropharyngeal lipomas have typical characteristics on CT and MRI and therefore imaging of these lesions is important for diagnosis but also for anaesthetic and surgical planning. On CT, they appear as well defined, non-enhancing, low attenuation (65–125 Hounsfield Units) homogenous lesions, as demonstrated in this case.4 5 The differential diagnoses of vallecular lesions include malignant tumours, benign vallecular cysts such as mucous retention cysts and dermoid or epidermoid cysts.5 A lipoma located in a different area of the upper aerodigestive tract, such as the larynx, should also be considered as a differential diagnosis for clinical presentations such as that described in this case.6
Due to the soft and mobile nature of these lipomatous lesions, there is a risk of prolapse into the oral cavity (figure 2) leading to total obstruction of the airway during induction of anaesthesia.7 Therefore, careful anaesthetic assessment is required for all suspected oropharyngeal lipomas with consideration of positioning and awake fibreoptic intubation techniques.

{kind=link}
{kind=link}
Prolapse of the lipoma into the oral cavity intraoperatively.
Patient’s perspective
I had had the symptoms for around 4 or 5 years by the time I finally got diagnosed.
Until then I had found myself going to a GP either annually or biannually with the same throat issues. It was a frustrating time because close friends and relatives (some of whom work within the NHS) continued to show concern about my voice changes but GPs up to that point were quite dismissive and twice gave me a nasal spray which was completely ineffective.
When I could feel a lump within my throat that was gradually increasing in size, it made me think that I had cancer or a tumour of some sort. This was obviously a very scary prospect.
Learning points
Patients with insidious onset of voice change should have flexible nasendoscopic assessment of their larynx.
Consider lipoma in the differential diagnosis of lesions of the vallecula.
Careful assessment and consideration of awake fibreoptic intubation is essential for large oropharyngeal lesions in order to prevent total airway obstruction during anaesthesia.
Footnotes
Contributors JL: patient care, and planning, design and writing of the case report. RM: patient care, and planning and revising of the case report. PM: patient care, and review and editing of the drafts. All authors were involved in the final approval for submission, including agreement to accountability for the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.