Article Text

Statistics from Altmetric.com
Description
A middle-aged former smoker with a medical history of chronic obstructive pulmonary disease (COPD) and idiopathic pulmonary arterial hypertension (IPAH) was transferred to our facility for management of a pulmonary artery aneurysm (PAA) found on CT scan of the chest. The patient was diagnosed with IPAH 13 years prior to current presentation and had been on dual pulmonary hypertension therapy (macitentan and sildenafil) with improvement in 6 min walking distance and functional class. At the outside facility, the patient was admitted for a respiratory tract infection and treated with antibiotics. A CT scan of the chest revealed pulmonary consolidation and PAA (figure 1).

CT scan showing evidence of right heart strain with a right pulmonary artery aneurysm measuring 54.1 mm with hypodensity suggesting intramural thrombus. Cross-section highlighting aneurysm and arrow pointing at intramural thrombus.
On admission to our centre, the patient’s blood pressure was 156/83 mm Hg, heart rate was 105 beats/min and oxygen saturation was 95% on 3 L/min oxygen by nasal cannula. Physical examination revealed a loud S2, a holosystolic murmur at the left sternal border, diffuse wheezing and lower extremity cyanosis and mild clubbing not noted in the upper extremities. Transthoracic echocardiogram revealed normal left ventricular function, moderately dilated and severely hypertrophic right ventricle with mildly decreased function and an estimated right ventricular systolic pressure of 97 mm Hg. A right heart catheterisation showed mean pulmonary artery pressure (PAP) of 98 mm Hg, cardiac output 9.27 L/min and pulmonary vascular resistance (PVR) of 8.6 wood units. Six-minute walk distance was 384 m with desaturation to 78% on room air. Pulmonary function testing showed forced expiratory volume in 1 second (FEV1) of 23% predicted, forced vital capacity (FVC) of 48% predicted, FEV1/FVC of 37% with a positive bronchodilator response. Haemoglobin was 159 g/L. CT scan of the chest revealed a right PAA 54.1 mm in anteroposterior diameter compressing the pulmonary vein and right bronchus, a right upper lobe consolidation and a patent ductus arteriosus (PDA) measuring 18.4 mm (figures 1 and 2). At the time of his presentation to our facility, outside records were not available.
{kind=link}
{kind=link}
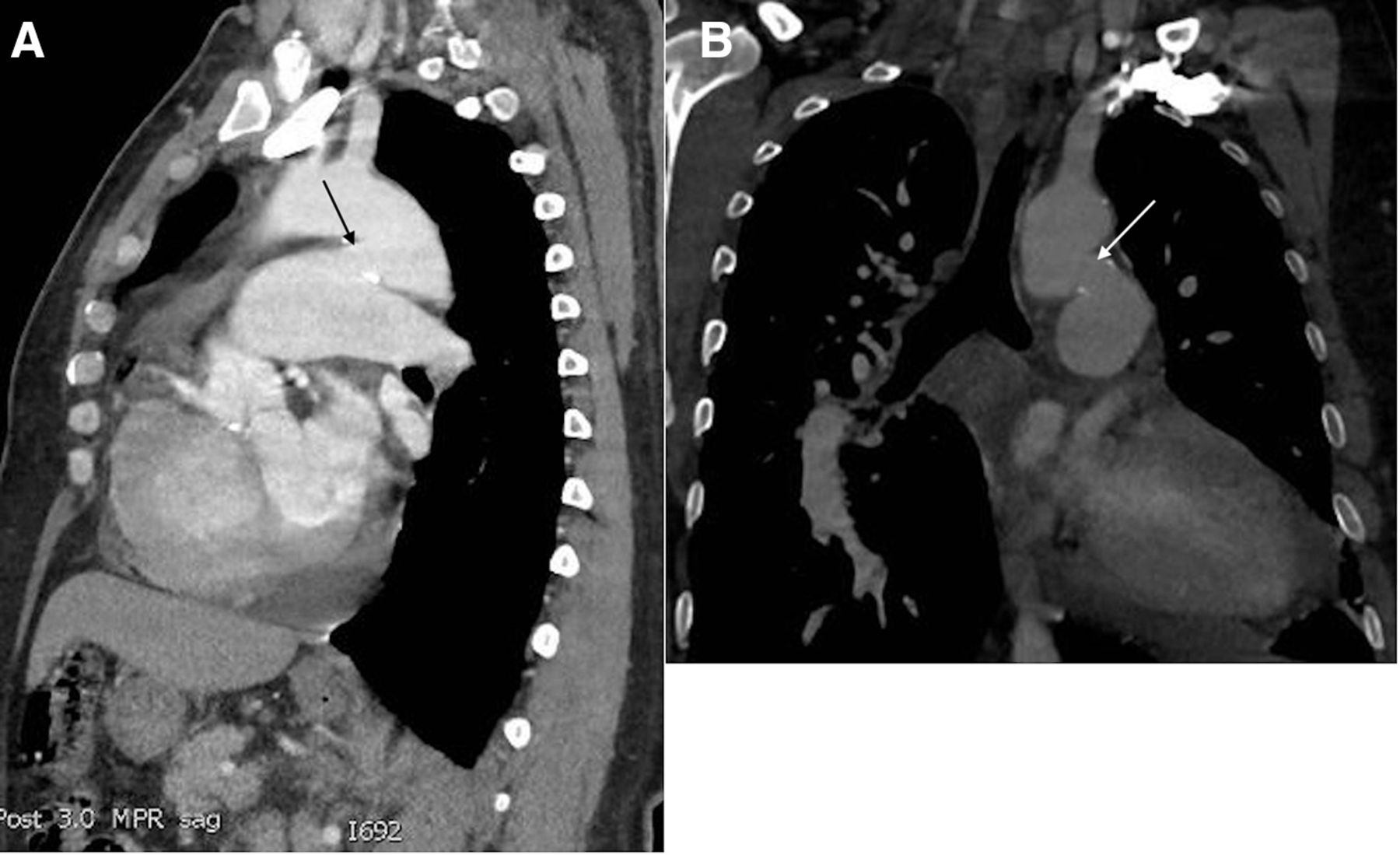
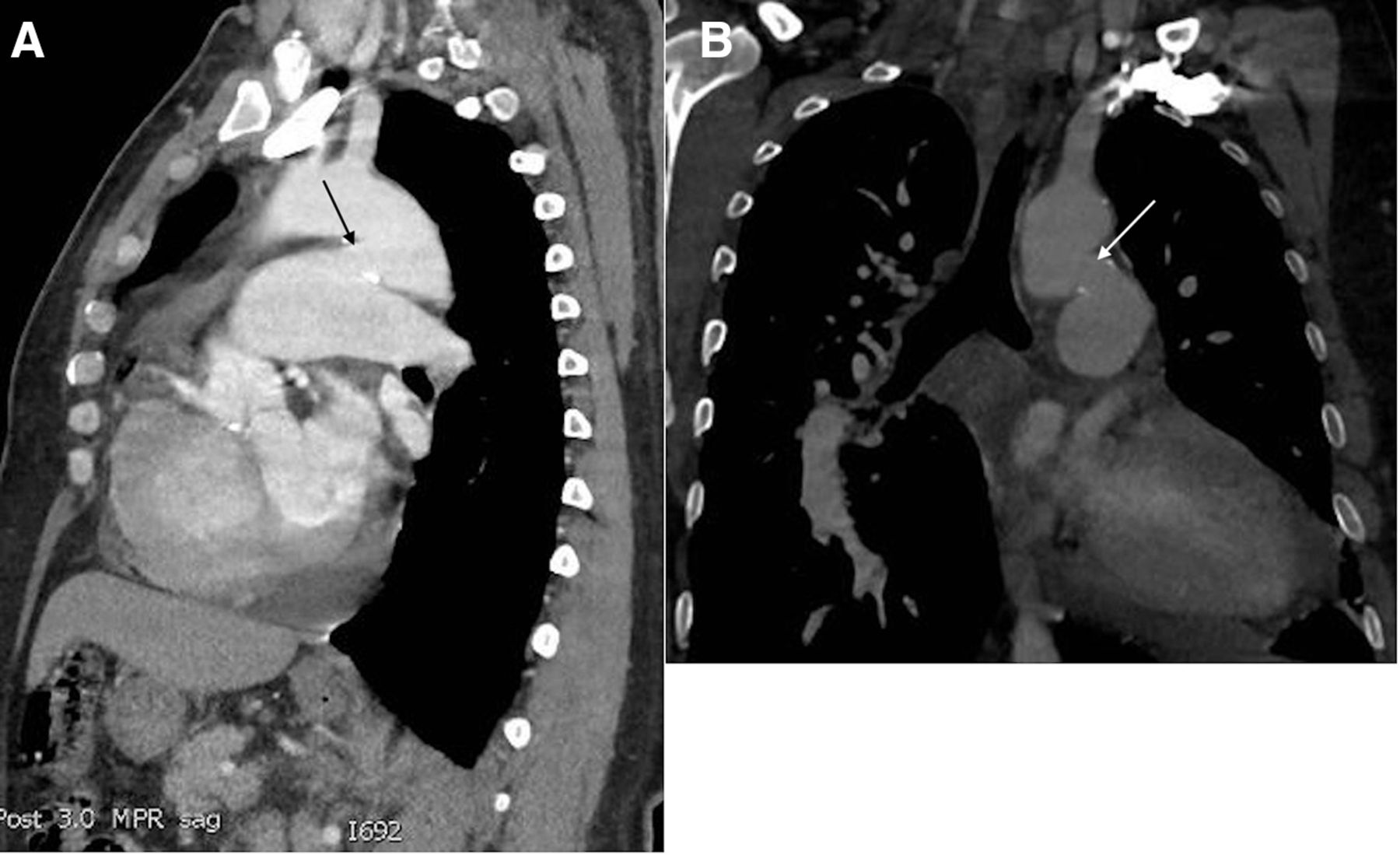
CT scan of newly identified PDA. (A) Wide PDA connecting the inferior surface of the descending aorta to main pulmonary trunk. PDA measures 18.4 mm. (B) PDA in the coronal plane. Arrows point at PDA. PDA, patent ductus arteriosus.
Based on the CT scan findings, PAH classification was changed to PAH associated with congenital heart disease (PAH-CHD). In view of the elevated PAP and PVR, surgical intervention was not offered. Our decision was to optimise medical management for PAH and COPD and have close follow-up.
PAH-CHD comprises 21% of WHO category 1 PAH.1 A PDA shunt lesion is identified in 1% of adults with PAH-CHD.2 As evidenced in this case, PDAs are easily missed on echocardiography, resulting in patients being misdiagnosed as IPAH. Additionally, congenital heart diseases have been recognised as the major reason for PAA formation with more than 50% of all cases associated with congenital heart defects. The most commonly associated lesions are PDAs, ventricular septal defects and atrial septal defects.3
In conclusion, our patient’s disease stability over 13 years and the findings of PAA were indicative of an associated congenital heart defect. This case demonstrates the challenges and nuance of working up pulmonary hypertension and the importance of thorough diagnostic procedures and imaging.
Learning points
The disease course of idiopathic pulmonary hypertension is progressive. Patients that remain stable for many years should be re-evaluated for underlying causes, in particular, associated congenital heart defects.
Half of all pulmonary artery aneurysms are associated with congenital heart disease. Identification of an aneurysm should prompt further imaging, especially in the presence of other signs of congenital heart disease.
Footnotes
Contributors KADD was responsible for the writing of the case report as well as the compilation, editing and preparation for submission. SF was responsible for planning, writing, editing and interface with the patient. ME assisted with selection, annotation and captioning of the images. HS planned, edited the text and provided cardiology perspective.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.