Article Text

Statistics from Altmetric.com
Description
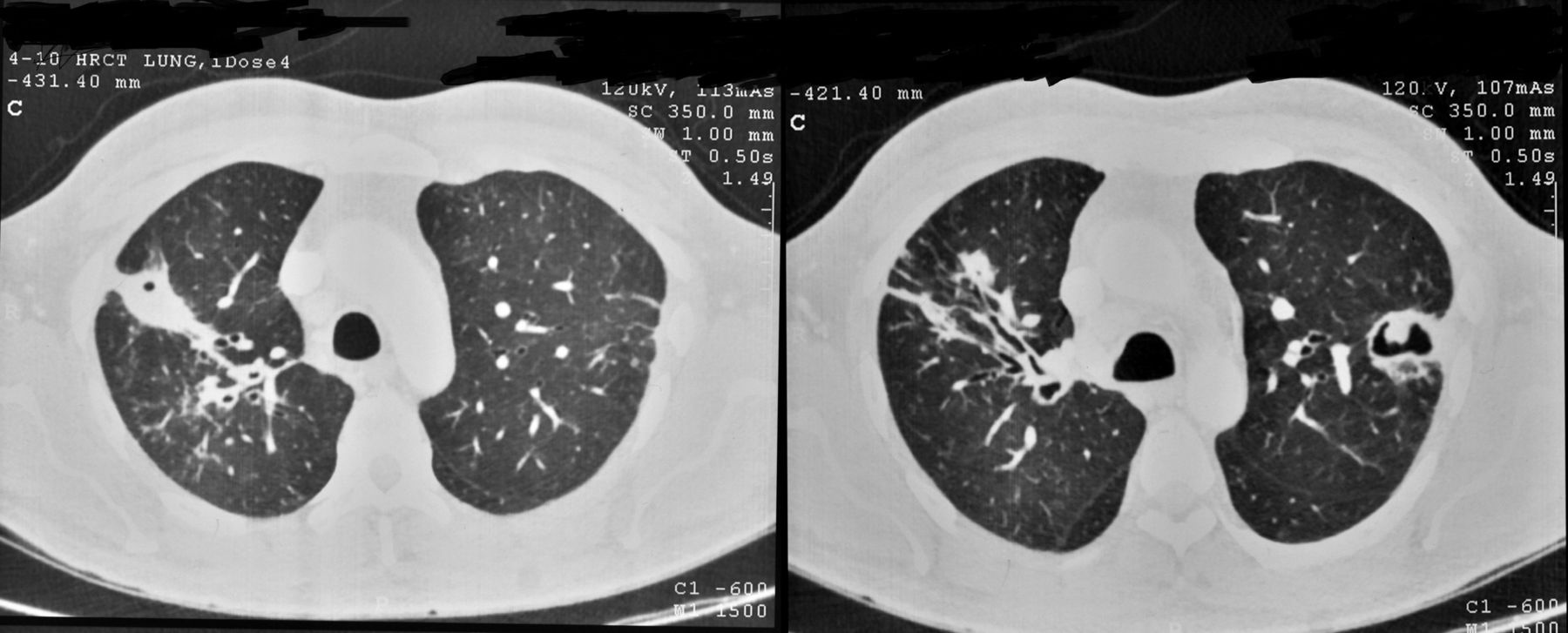
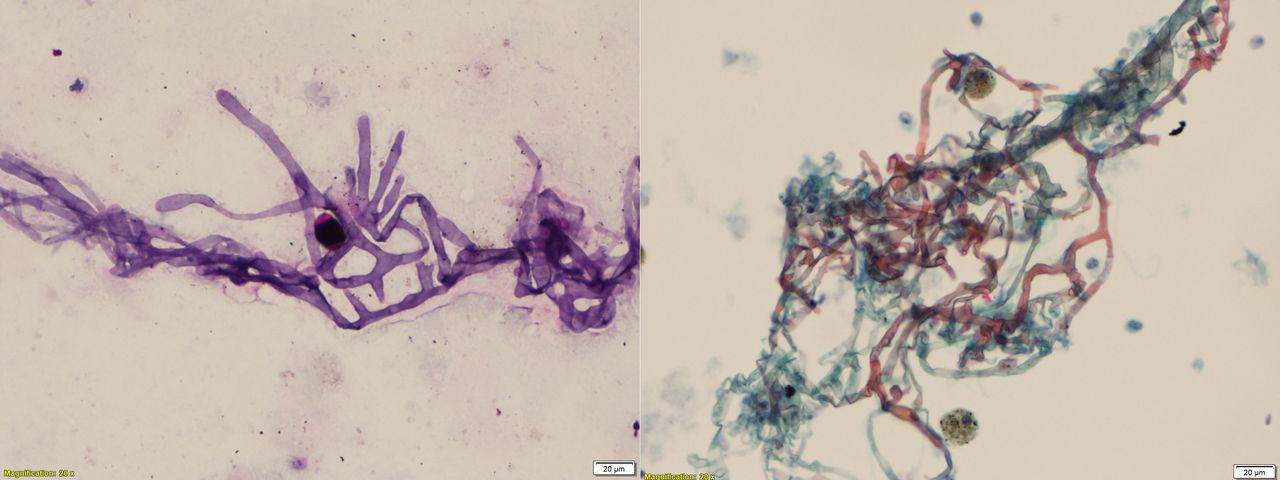
A 45 -ear-old man presented with complaints of cough with minimal expectoration for 3 months. He was a known case of type 2 diabetes mellitus for the past 2 years. His complete blood count, renal function and liver function tests were within normal limits. His haemoglobn A1C was 8.2%. There were no features suggestive of neuropathy, nephropathy or retinopathy. His chest radiograph was showing bilateral heterogeneous opacities in upper zones. Sputum acid fast bacilli (AFB) and culture were negative. High-resolution CT of chest (figure 1) revealed bilateral central ground glass opacities surrounded by dense consolidation suggestive of reverse Halo sign. Bronchoalveolar lavage fluid cytological examination showed the presence of broad aseptate hyphae (figure 2) suggestive of mucormycosis. A diagnosis of pulmonary mucormycosis was made, and he was treated with amphotericin B. Repeat CT showed improvement in the original lesions (figure 3).

Pretreatment high-resolution CT of thorax showing reverse halo sign represented by central ground glass opacity and surrounding dense consolidation in right upper lobe (arrows) with additional similar lesions in both upper lobes.

H&E and Gomori methenamine staining of the bronchoalveolar lavage sample showing aseptate broad hyphae with acute angle branching and self-folding at places in ×20 magnification suggestive of mucormycosis.
{kind=link}
{kind=link}
{kind=link}
Post-treatment high-resolution CT images of the same lesions showing improvement with residual fibrosis and traction bronchiectasis in the right upper lobe and residual cavity with intracavity content in the left upper lobe.
The presence of uncontrolled blood sugar levels is an independent risk factor for fungal infections in patients with diabetes.1 Mucorales order consists of ubiquitous organisms commonly growing on decaying vegetables and soil. The genera found in human are Rhizopus, Mucor and Cunninghamella and Apophysomyces. Most common sites of involvement are rhinocerebral, pulmonary and renal. The hyphae of Mucorales are distinct with characteristic features like broad (5–15 µm), irregularly branched, acute-angled and predominantly aseptate.2
Reverse halo sign or atoll sign has been associated with diseases like pulmonary mucormycosis, tuberculosis, cryptogenic and secondary organising pneumonia, paracoccidioidomycosis and pulmonary thromboembolism. The first description of atoll sign was given in cryptogenic organising pneumonia, where the central ground glass opacity represents clearing of the inflammation with residual alveolar septal inflammation, and the denser outer rim denotes granulation tissue filling the alveolar air spaces.3 4 Reverse halo sign (RHS) in fungal infections is due to infarct with haemorrhage which is greater at periphery than at the centre. This is denoted by the fact that in subsequent CT, our patient had a newly formed cavity at the site of the original RHS. This is an indirect sign of vascular invasion by the fungal infection. Central cavitation and residual lesions denote that the mechanism of RHS in mucormycosis is haemorrhagic central infarction due to vascular invasion. Cavitation after RHS in mucormycosis is seen only in a minority of cases after complete treatment.
Learning points
Uncontrolled diabetes mellitus is an important risk factor for pulmonary mucormycosis.
Reverse halo sign is an important radiological finding of pulmonary mucormycosis.
Treatment with amphotericin B improves clinical and radiological outcomes.
Footnotes
Contributors Both authors, PKS and PS have contributed equally in planning, conducting and writing of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.