Article Text

Statistics from Altmetric.com
Description
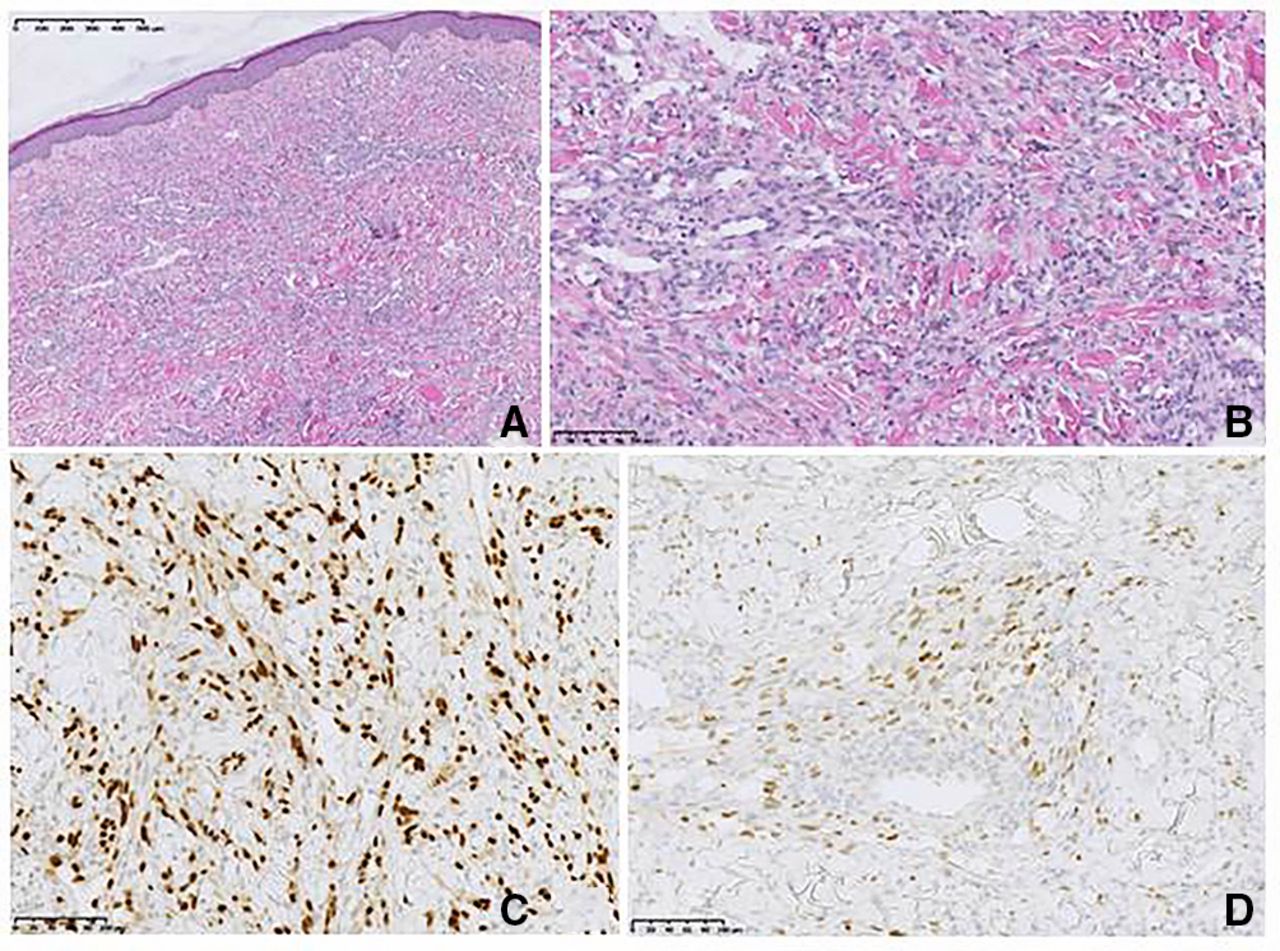
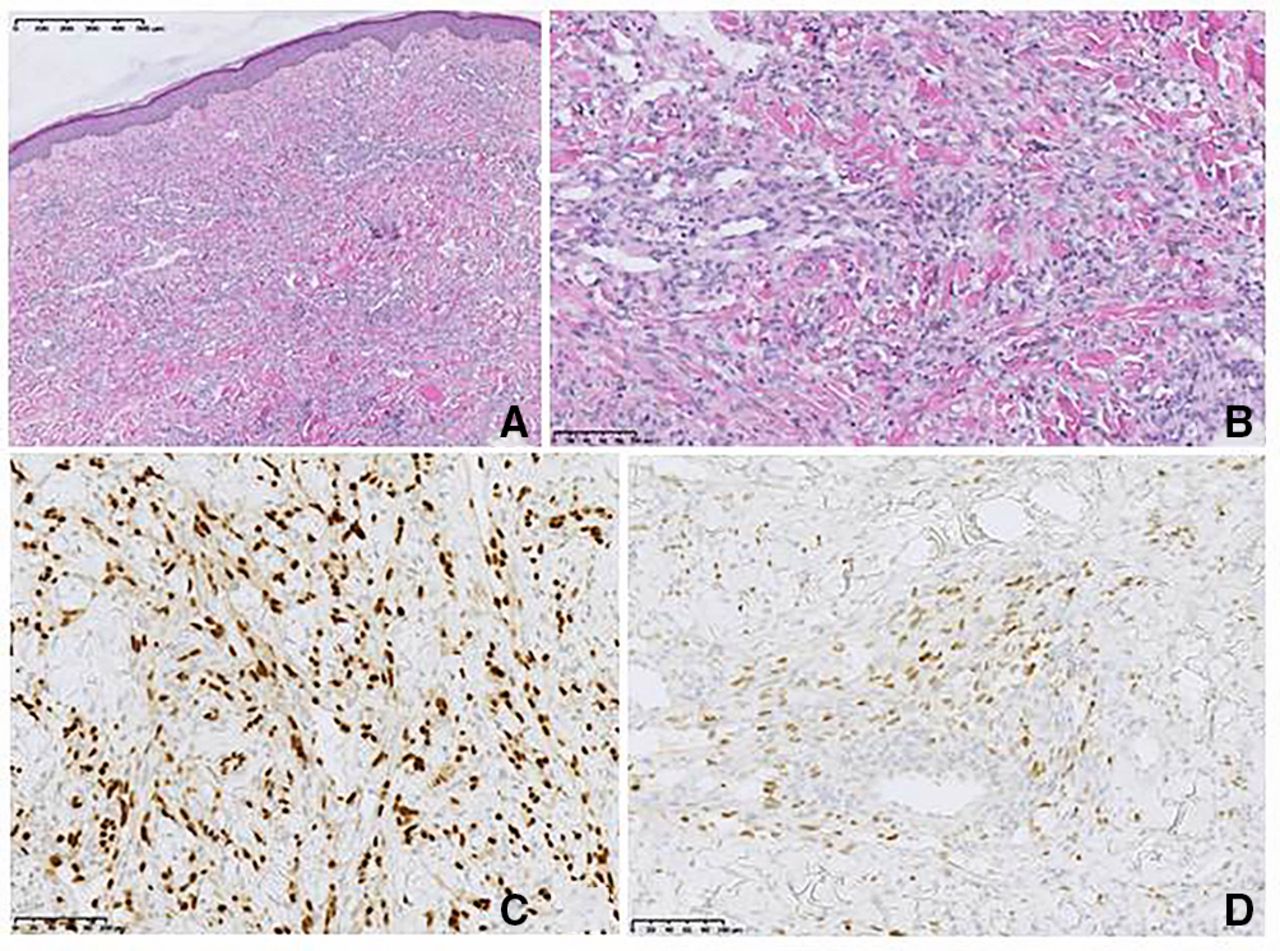
A North-African woman in her mid-70s presented with a red-purplish macular rash on her right thigh and left lower limb. The skin lesions had developed over the last 6 months and did not cause pruritus or pain. She had been transplanted with a deceased-donor kidney 5 years ago for diabetic nephropathy. Her treatment included tacrolimus, mycophenolate mofetil (MMF) and low-dose methylprednisolone. Physical examination revealed large cutaneous purplish confluent infiltrative plaques on the anterior left leg and right thigh highly evocative of Kaposi sarcoma (KS) (figure 1A). No ulceration, bleeding or oedema was noted. Regional lymph nodes were not palpated. Laboratory tests were in the usual range. HIV serology was negative. Skin biopsy confirmed the diagnosis of KS: histology revealed the presence of fusiform cells of endothelial origin and neovessels (figure 2A,B), while immunohistochemical staining showed positive labelling for erythroblast transformation-specific related gene (ERG) and human herpes virus type 8 (HHV8) on endothelial cells (figure 2C,D). Positron-emission tomography did not reveal hyper metabolic lesions. Chemotherapy based on pegylated liposomal doxorubicin (PLD), cessation of MMF and a switch from tacrolimus to sirolimus was proposed. The patient declined the treatment and left the country. She came back 1 year later with significant spread of skin lesions (figure 1B). She received five cycles of PLD without improvement, and was quickly readmitted for general weakness, anorexia, epigastralgia, dysphagia and cough. Workout revealed interstitial pneumonitis, esophagitis and gastric ulcer. Bronchoalveolar lavage was not contributive, but immunohistochemistry of the gastric lesion revealed an atypical vascularisation positive for HHV8 and ERG, compatible with KS. The patient became rapidly hypoxic and died.

Skin lesions in Kaposi sarcoma. (A) Large cutaneous purplish confluent infiltrative plaques on the anterior left leg and right thigh. (B) Significant spread of skin lesions.
{kind=link}
{kind=link}
Histological and immunohistochemical features of Kaposi’s sarcoma. Histological section showing fusiform cells and neovessels ((A) H&E ×5 and (B) H&E ×20). (C) Erythroblast transformation-specific related gene labelling, endothelial differentiation marker (×20). (D) Positive labelling for HHV8 (×20). HHV8, human herpes virus type 8.
KS is an angioproliferative cutaneous cancer caused by human herpesvirus 8.1 Skin lesions are typical and make the diagnosis. These are purple-red-bluish lesions presenting as non-painful, non-itchy, macules, papules, plaques or nodules. Due to their vascular aetiology, they can ulcerate and bleed. The incidence of KS is higher in transplant patients than in non-immunosuppressed populations. In kidney transplant recipients, the intensity and duration of immunosuppression, and the presence of HHV8 serology pretransplantation increase the risk of developing KS, which occurs 13 months after transplantation (range few weeks to 18 years).2 Serological testing for HHV8 was unavailable pretransplantation for our patient and the donor, making difficult to ascertain the origin of the infection. However, the Mediterranean origin of the patient where HHV8 seroprevalence is high made her at risk for KS. Lesions usually begin on the lower limbs, with multifocal and asymptomatic development. KS may remain localised to the skin, but dissemination to visceral mucosa of the trachea, lungs and gastrointestinal tract is common in immunosuppressed patients. Reduction of immunosuppressive therapy, as well as a switch of calcineurin inhibitor to mammalian target of rapamycin may obtain resolution of disease in the early stages of the disease.3 For extensive involvement, liposomal anthracyclines is proposed as a first-line therapy.4 Mucosal dissemination or visceral involvement has usually a poor prognosis.2 Our patient refusal of treatment for 1 year contributed to the dramatic spread of KS and fatal outcome.
Learning points
Kidney transplant recipients are at higher risk of Kaposi sarcoma because of immunosuppression and human herpes virus type 8 reactivation.
Dissemination is common if not treated rapidly and adequately.
A late diagnosis with visceral involvement has a poor prognosis.
Footnotes
Contributors JR wrote the first draft. LM took care of the patient. AC did the histology analysis. NK took care of the patient and wrote the final draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None decared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.