Article Text

Abstract
We present a case report of anomalous mitral arcade in a live born former recipient of twin–twin transfusion syndrome. At 33+0 week of gestation fetal ultrasound demonstrated that she had a large mitral insufficiency, decreased movement of the lateral cusp of the mitral valve and dilated left atrium. The twins were delivered by caesarean section at week 33+1 due to fetal distress. The former recipient twin developed decompensated heart failure during her first day of life and was transferred to a surgical paediatric heart centre. Her clinical condition rapidly deteriorated, and she died of congestive heart failure 3 days old. Prenatal signs of anomalous mitral arcade in a recipient of twin–twin transfusion syndrome should warrant preparation of a critically ill neonate, including parental counselling and in utero transfer to surgical paediatric heart centre. There is a surgical treatment option available for neonates, but the experience with this technique is still very limited with a high risk of morbidity and mortality.
- heart failure
- valvar diseases
- neonatal intensive care
- obstetrics and gynaecology
- ultrasonography
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Twin–twin transfusion syndrome affects 10%–15% of all monochorionic twin pregnancies.1 The cause is an unbalanced transfusion of fluid and vasoactive mediators from one twin to the other, through placental anastomoses. In the recipient twin, this could lead to hypertension, congestive heart failure and hydrops fetalis.1
Recently a rare valve deformity called anomalous mitral arcade was found in recipient twin–twin transfusion fetuses that had died in utero.2 Anomalous mitral arcade can give mitral insufficiency and stenosis, and is associated with a high risk of early death.3 It has never been reported in a live born recipient of twin–twin transfusion syndrome.
Case presentation
A 35-year-old secundigravida with monochorionic diamniotic twins diagnosed with twin–twin transfusion syndrome presented at Rikshospitalet, Oslo in week 17+2 of gestation. Selective fetoscopic laser photocoagulation was performed in Hamburg in week 18 of gestation. Signs of decreased heart function in twin 1 (former recipient) were noted on ultrasound 27+2 weeks of gestation. This was confirmed in week 28+0 of gestation, as reduced contractility of the myocardia, thickening of the myocardium, as well as mitral and tricuspid insufficiency. She was admitted at Rikshospitalet due to preterm prelabour rupture of membranes in 31+2 weeks of gestation. Due to capacity problems at Rikshospitalet, she was transferred to St. Olavs Hospital in Trondheim for further care in week 31+5 of gestation.
Fetal echocardiography at St. Olavs hospital in gestational week 33+0 revealed a large mitral insufficiency, decreased movement of the lateral cusp of the mitral valve, and a dilated left atrium (figure 1, videos 1 and 2) in twin 1. Since this is an atypical presentation of heart failure in twin–twin transfusion syndrome, the relevant literature was reviewed, yielding the tentative diagnose of anomalous mitral arcade. Furthermore, the fetuses showed increasing signs of fetal distress. Twin 2 was tachycardic and growth restricted. In utero transfer back to the surgical paediatric heart centre in Norway (Rikshospitalet) was discussed, but not possible due to capacity problems. The twins had to be delivered with caesarean section in week 33+1. Prenatal steroids were administered before delivery.
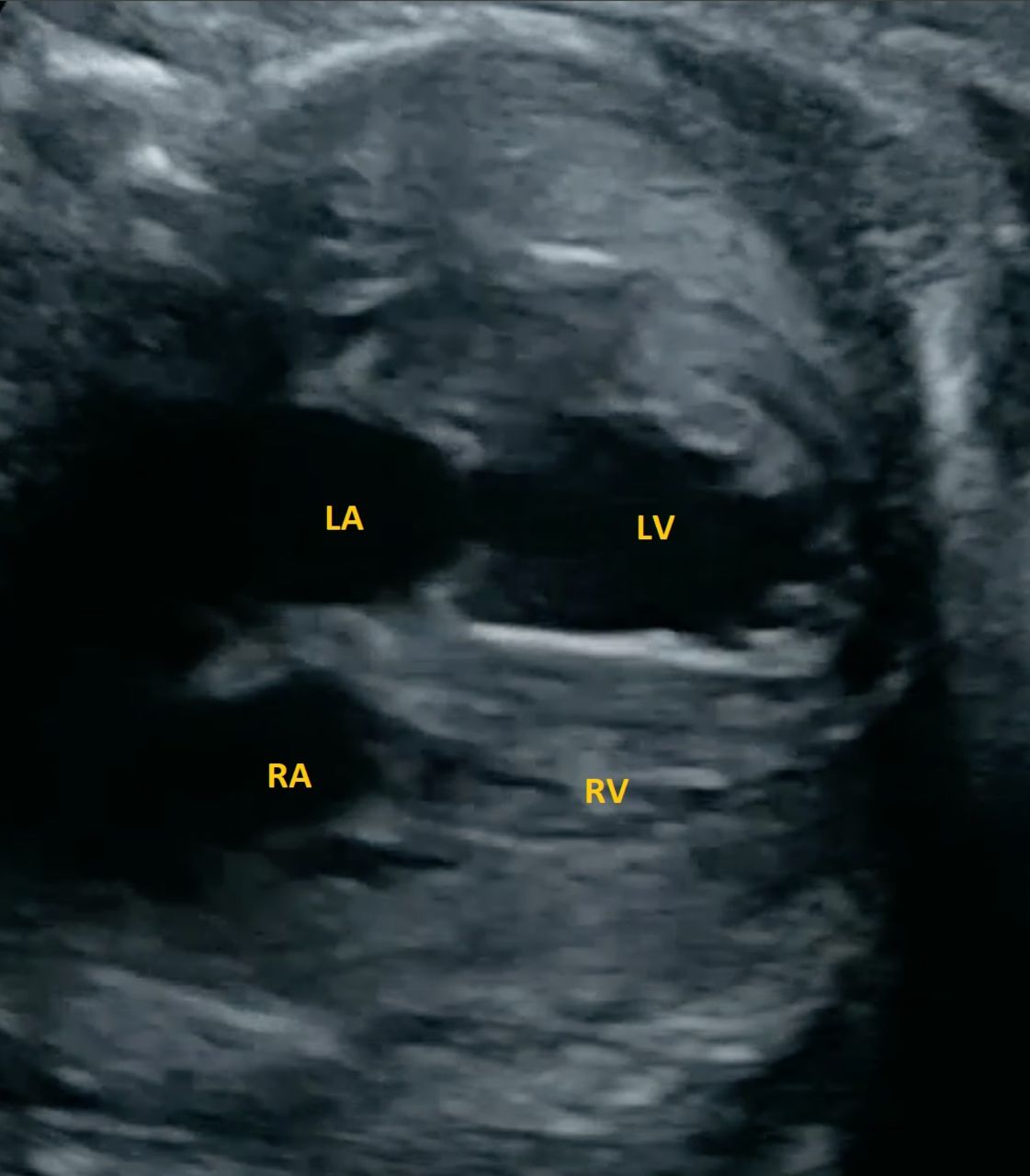
A four-chamber view of the fetal heart, demonstrating an enlarged heart with a dilated left atrium and biventricular hypertrophy. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
A four-chamber view of the fetal heart, demonstrating an enlarged heart with a dilated left atrium, left ventricular hypertrophy, and decreased movement of the lateral cusp of the mitral valve.
A four-chamber view of the fetal heart, demonstrating a large mitral insufficiency.
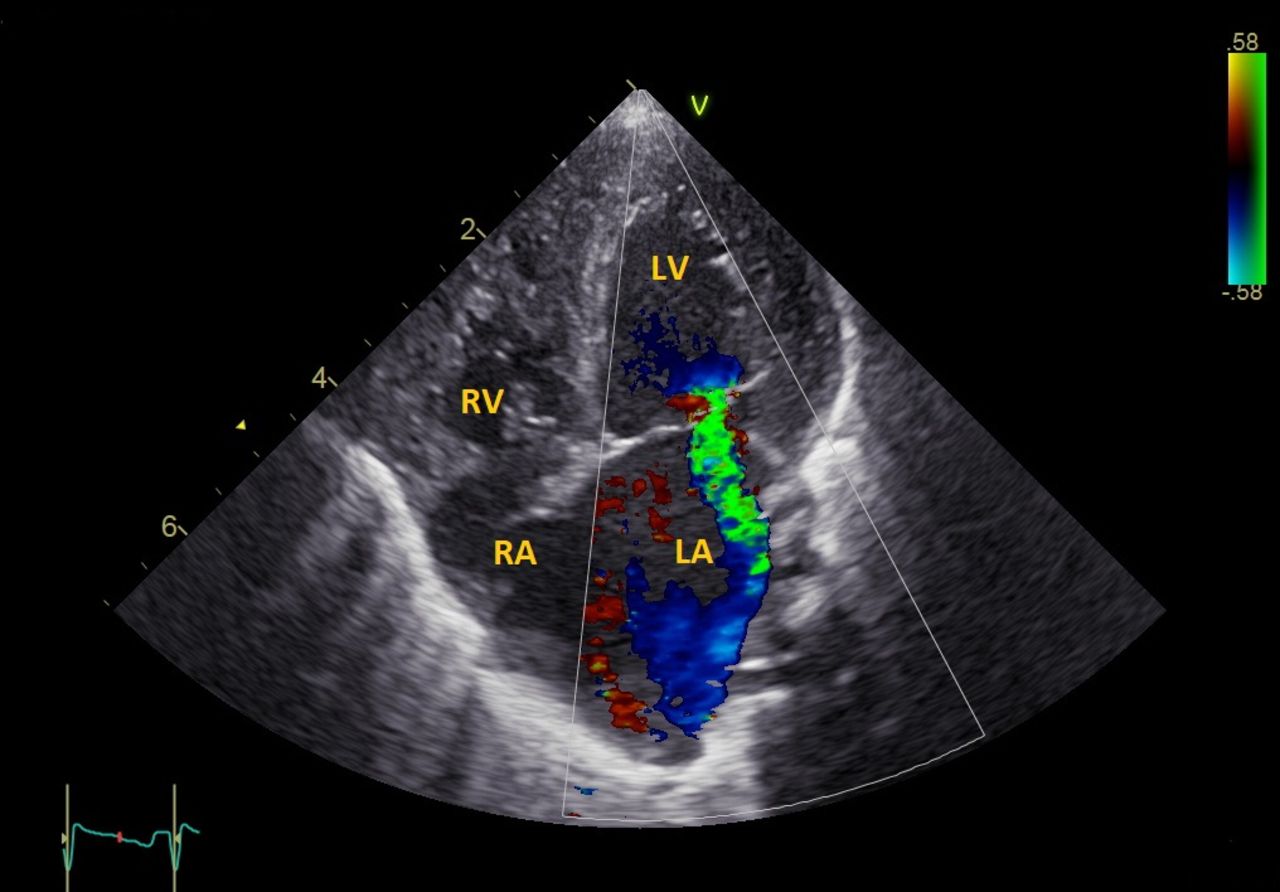
Twin 1 weighed 2000 g, and received an Apgar score of 5–7–8. She presented with mottled skin, a systolic murmur grade 3/6 and hyperactive precordium. She was intubated 45 min after birth due to respiratory failure. After intubation her skin colour improved and she no longer required oxygen supplement. Echocardiography after birth confirmed the diagnosis of anomalous mitral arcade with dilated left atrium, left ventricular hypertrophy, mitral stenosis (mitral valve area 0.4 cm2) and insufficiency (figures 2 and 3, video 3) and short chordae tendinae (figure 3, videos 4 and 5). She showed signs of elevated pulmonary resistance (estimated pulmonary pressure of 57 mm Hg), with right to left shunt across a patent ductus arteriosus. Chest X-ray showed an enlarged heart and prominent pulmonary vessels. She was stable in terms of circulation during her first day of life, but became hypotensive on day 2, and a dopamine infusion was started. Her blood pressure normalised, but she showed increasing signs of impaired organ perfusion. She was transferred to Rikshospitalet by air ambulance, and perceived as stable during transfer.

A four-chamber view of the neonatal heart, demonstrating an enlarged heart with a dilated left atrium, biventricular hypertrophy, and a stenotic and regurgitant mitral valve. LA, left atrium; LV, left ventricle; RA=right atrium; RV, right ventricle.

A parasternal short axis view of the heart, demonstrating biventricular hypertrophy and short chordae tendinae. LV, left ventricle; MV, mitral valve; RV, right ventricle.
A four-chamber view of the neonatal heart, demonstrating an enlarged heart with a dilated left atrium, biventricular hypertrophy, and a stenotic and regurgitant mitral valve.
A parasternal long axis view of the heart, demonstrating short chordae tendinae.
A parasternal short axis view of the heart, demonstrating left ventricular hypertrophy and short chordae tendinae.
On arrival, her clinical condition deteriorated significantly. She had tachycardia, prolonged capillary refill time, enlarged liver and a systolic murmur grade 4/6 with apparent chest thrill. It was difficult to palpate the femoral pulses, and her right leg was cold to touch and profoundly discoloured. Chest X-ray showed pleural effusion. Findings on echocardiogram were dominated by a significant mitral insufficiency, overall reduced contractility, as well as pleural and pericardial exudates. Since the main cause of the heart failure was mitral valve insufficiency, there are few available pharmacological treatment options. Inotropic support with Dopamine was ongoing. Milrinone was started to increase myocardial contractility and reduce afterload. Fluid boluses were administered with the rationale to try to increase left ventricular output and subsequently improve organ perfusion. However, we cannot rule out that the administration of fluid boluses may also have increased the fluid congestion in the pulmonary circulation in this patient. The pericardial effusion increased the same night, which lead to circulatory collapse. Cardiopulmonary resuscitation including pericardiocentesis and pleurodesis was performed. Return of spontaneous circulation was established after 6 min. Afterwards she was severely hypotensive. Epinephrine infusion was started, which gave amended contractility.
Outcome
Her condition and therapeutic options were discussed in an interdisciplinary team including thoracic surgeons, paediatric cardiologists and neonatologists. It was concluded that there was no surgical option available to alleviate her mitral valve incompetency at that time. Furthermore, there were no medical treatment options available that would prolong her life long enough to receive heart surgery at a later stage. ECMO was discussed, but due an overall assessment of the patient’s dire prognosis, age and size, it was not offered. She received palliative care and died 3 days old. The post mortem examination confirmed that she had hypertrophic heart with stenotic mitral ostium with small mitral valve cusps and dilated left atrium. Furthermore, a pale endocardial surface of the heart was observed (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A pathology specimen picture of the recipient’s heart, demonstrating thickening of the left ventricle with pale endocardial surface, and a narrow mitral valve with small papillary muscles and almost absent tendinous cords. LV, left ventricle; MV, mitral valve.
Discussion
This is the first reported case of anomalous mitral arcade in a live born former recipient of twin–twin transfusion syndrome. The first signs of heart failure were seen several weeks after laser therapy. It is important to be aware of the prenatal ultrasound signs of anomalous mitral arcade, as it can imply a critical condition with high risk of early death.
The haemodynamic strain of volume overload and increased peripheral resistance in the recipient twin of twin–twin transfusion syndrome is significant, and at time of diagnosis up to 70% of fetuses show signs cardiac compromise.1 Selective fetoscopic laser photocoagulation is the only specific treatment available for twin–twin transfusion syndrome,1 and normally gives a rapid improvement in heart function.4 Our case had an unusual presentation of heart failure, after laser treatment for twin–twin transfusion syndrome, including a serious malfunction of the mitral valve. Recently a rare mitral valve deformity called anomalous mitral arcade was found to be associated with twin–twin transfusion syndrome.2 In 11 sets of autopsied twin–twin transfusion syndrome fetuses, that had died in utero, anomalous mitral arcade was found in four recipient twins. Anomalous mitral arcade was associated with prenatal findings of left atrial dilation, mitral insufficiency and decreased leaflet mobility in recipients, similar to the present case.2
Anomalous mitral arcade is recognised by a bridge of fibrous tissue arched between the two papillary muscles, as well as an abnormal relationship between the papillary muscles and valvular leaflets.3 The pathogenesis is poorly understood.2 Previously the malformation was thought to result from an arrest in the development of the mitral valve, at a stage after loss of muscle in chordae and leaflets, but before the final attenuation and elongation of mitral chordae have occurred.3 The fibrous ridge across the free margins of the mitral leaflet was thought to be a remnant of a developing leaflet.3 However, recent findings challenge these previous assumptions and suggest that anomalous mitral arcade is an acquired deformity.2 If this is true, the fibrous ridge might represent remodelling of the valve complex due to turbulent blood flow across the mitral valve.2 Specifically, Losada et al 2 suggest that anomalous mitral arcade in the recipient twin of twin–twin transfusion syndrome can be caused by the hemodynamically strains on the mitral valve.
The clinical presentation of anomalous mitral arcade is usually mitral insufficiency and/or mitral stenosis and severe congestive heart failure.5 The diagnosis is made by echocardiography, with characteristic findings that can even be seen in utero.2 6 Early mortality is high and survival into adulthood is rare, but reported.2 5–15 The available treatment options are limited, and although technically challenging, mitral valve repair is the preferred method.7–9 15 There are case reports of successfully performed mitral valve replacement from 6 months of age7 8 and mitral valve repair from teenage years.9 15 Recently Pluchinotta et al 16 reported a multicentre study of surgical implantation of the Melody bioprosthetic valve in mitral position for children and infants with intractable mitral disease as early as the neonatal period. The median age and weight at implantation was 8.6 months (range 3 days to 14 years) and 6.6 kg (range not reported), respectively.16 The experience with this technique is still very limited, and in a preterm neonate weighing only 2 kg there would probably be only a minimal chance ofgain.16
In conclusion, prenatal ultrasound findings supportive of anomalous mitral arcade in a former recipient of twin–twin transfusion syndrome, should warrant preparation for a critically ill neonate, including parental counselling and in utero transfer to a surgical paediatric heart centre. There is a surgical therapeutic option available for infants, but the experience with this technique is still very limited with a high risk of morbidity and mortality.
Patient’s perspective
I remember my pregnancy as a living nightmare. I knew early in the pregnancy that I was expecting twins. I read a lot about twin pregnancies, including the risk of twin–twin transfusion syndrome. When it was discovered that the girls had this condition, the centre of fetal medicine at Rikshospitalet took over the responsibility for me. I was sent to Hamburg. During these weeks, I felt well looked after.
Throughout the pregnancy, I felt ill with pruritus, nausea and sleep problems. In addition, I was often on ultrasound scans, with little encouraging news. It was a though pregnancy. I was worried about the girls all the time.
We were told that twin 1 (recipient) might need heart medicine, and even heart surgery. The doctors were still most worried about twin 2 (donor). Several times, they said that things did not look good for her. In gestational week 26, we were told that we had to go back to Hamburg to cut twin 2’s placental cord. Two days later, we were told that the procedure could not be performed anyway. It was too risky. I do not think words can describe how I felt.
I was strongly against the transfer from Rikshospitalet to St. Olavs Hospital. I have never understood that I, pregnant with a heartsick baby, could be sent away. I wanted to give birth at Rikshospitalet. They had taken care of me during the pregnancy, and I knew this hospital was well equipped to take care of a child with a heart condition. It was also important for me to have my son and husband with me. It was sadly out of my control. They promised me that it was only for the weekend, due to lack of space, but I stayed at St. Olavs Hospital for 10 days against my own wish. I called Rikshospitalet every day, asking to be sent back. The doctors at St. Olavs expressed the uncertainty in the situation, and I felt that they also wanted to transfer me back. At this time, my son was almost 3 years old, and it was painful not to be with him. My husband did not get to be there for the delivery. He arrived shortly after.
The transfer back to Rikshospitalet felt chaotic, and I experienced that the personnel had limited information about our situation. Among other things, I was never told that twin 2 did not leave for Oslo at the planned time. I searched for her the first night and I could not find her. I asked where she was, but very few knew what had happened and when she would arrive.
The time I had with twin 1 was full of grief, and sadly, I cannot have those days back. I was not able to think clearly, the contrasts got to big, and I felt there was so much disturbance and chaos around me. I was encouraged to hold my girl. However, it was almost impossible to make it happen. It had to be planned, and it was postponed several times. I had to go to another ward to pump breast milk for twin 2, and when the doctors went on rounds to see twin 1, I had to leave. I feel that the only and precious time that I had with her, was taken from me due to the bad organisation of the ward.
I wish that so many things had been different. I am disappointed in the Norwegian healthcare system. It is unbelievably painful to lose a child. We were also worried about our little dys- and premature girl, weighing 900 g. In addition, we had to endure what we did. It felt wrong and unfair. My husband and I have been back to Rikshospitalet for a conversation afterwards. The health clinic where we live, have offered us counselling with a psychologist, but we have not taken up the offer.
Note: This text has been translated from the mother’s native language into English. The twin’s names have been replaced with ‘twin 1’ and ‘twin 2’.
Learning points
There is an increased risk of anomalous mitral arcade development in the recipient of twin–twin transfusion syndrome.
Anomalous mitral arcade is important to recognise since it may have prognostic significance, with high risk of early mortality.
Anomalous mitral arcade should be suspected if prenatal ultrasound demonstrates left atrial dilation, mitral insufficiency and decreased leaflet mobility.
Suspicion of anomalous mitral arcade in recipient twin of twin–twin transfusion syndrome should warrant preparation of a critically ill neonate, including parental counselling and in utero transfer to a surgical paediatric heart centre.
Acknowledgments
We are most thankful for the contributions from: Aage Erichsen MD PhD, Department of Pathology Oslo University Hospital for taking the pathology specimen picture. Sigrid Bjørnstad MD, PhD, Department of Pathology Oslo University Hospital for providing us the pathology specimen picture as well as the interpretation of the findings. Christina Vogt, MD, PhD, Department of Pathology St. Olav’s Hospital for fruitful discussion regarding the pathology specimen picture.
Footnotes
Contributors All authors have each made a substantial contribution and qualify for authorship. The final version of the manuscript has been evaluated. Involved in the patient’s care: SAN, BK and AML. Conception and design: SAN and SSØ. Acquisition of data: the data material includes the patients’ medical journal as well as medical images. SAN, BK and AML provided access to the data material. SAN and SSØ have communicated with the patient’s parents to get consent and the parent’s perspective. Analysis and interpretation of data material: SAN and SSØ. Drafting the manuscript: SSØ. Revising the manuscript: SAN, BK, AML and SSØ have all been involved in revising the manuscripts for important intellectual content. All authors have contributed to the manuscript in a substantial way. Final approval of the version published: SAN, BK, AML and SSØ have all approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Parental/guardian consent obtained.