Article Text

Statistics from Altmetric.com
Description
Wilson’s disease, also known as hepatolenticular degeneration, is an autosomal recessive genetic disorder of copper metabolism leading to copper accumulation in many tissues, mainly the liver, brain, cornea and kidney. Copper deposition leads to specific hepatic, neurological, psychiatric and ocular signs and symptoms. The ocular manifestations of Wilson’s disease include Kayser-Fleischer ring (K-F ring) and sunflower cataract. K-F ring is almost always bilateral, starts superiorly first and then inferiorly, and later becomes circumferential.1 It results due to extracellular copper deposition in the Descemet’s membrane of the cornea.2
A 13-year-old male patient presented with gradually progressive, diminution of vision in both eyes. At presentation, the visual acuity was 6/24 and 6/18 in the right and left eye, respectively. Anterior segment examination revealed bilateral characteristic copper-coloured green–brown K-F ring near the limbus (figure 1A,B) along with yellow–brown opacities in the subcapsular cortex of the lens and pupillary zone with petal-like spokes suggestive of sunflower cataract (figure 2).3 Fundus examination was normal in both the eyes. Anterior segment ocular coherence tomography revealed hyper-reflective band at the level of Descemet membrane (DM) (figure 1C,D). Pentacam map revealed increased peripheral corneal thickness. Based on these findings, a presumptive diagnosis of Wilson’s disease was made, and the child was referred for systemic evaluation. The diagnosis of WD was confirmed with the presence of decreased ceruloplasmin, increased 24-hour urinary copper excretion and genetic analysis confirmed mutation of ATP7B gene. The child was managed with systemic D-penicillamine and a low-copper diet.
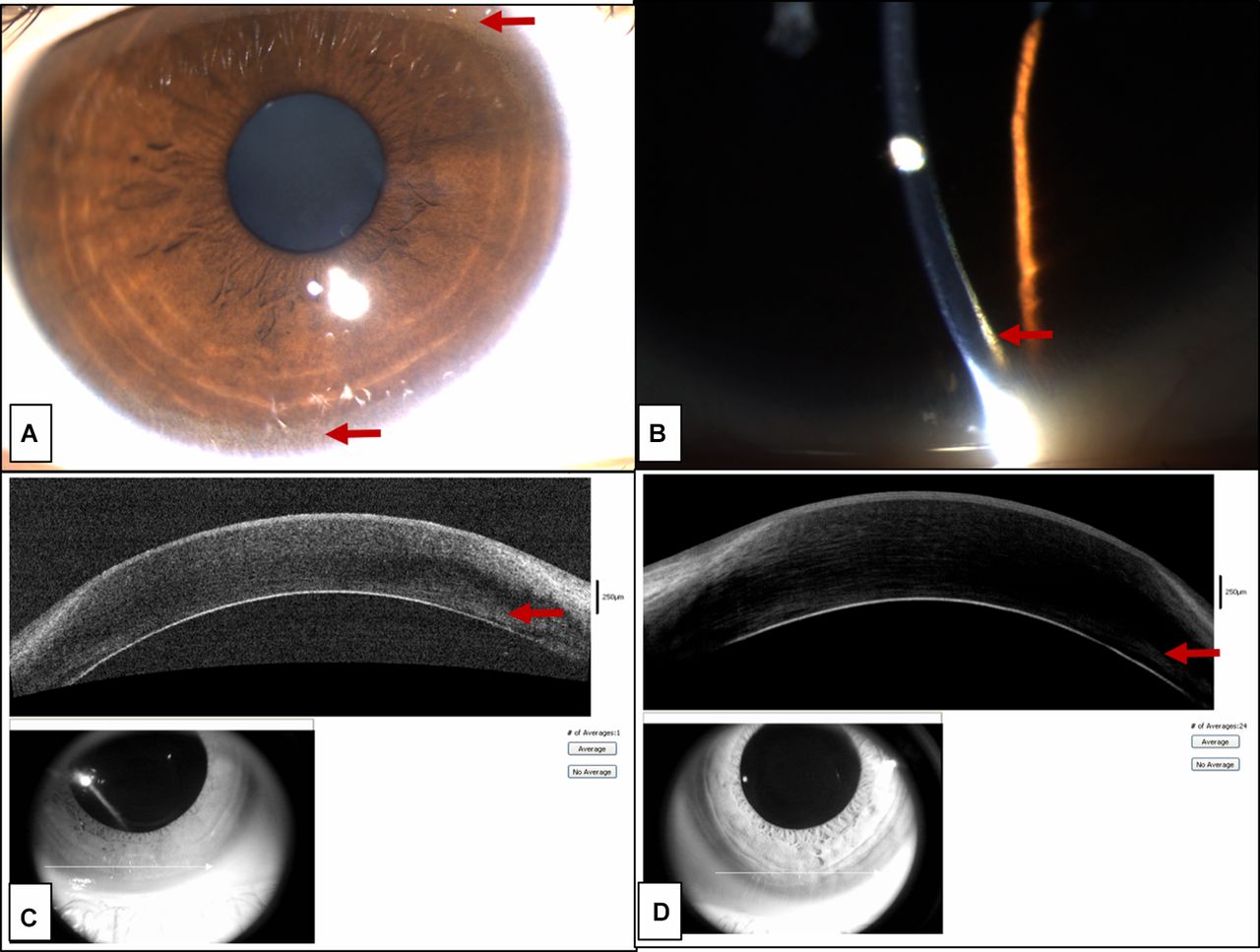
Slit lamp image of the right eye (A) diffuse illumination and (B) slit illumination showing green–brown copper deposition at the level of DM (K-F ring) (highlighted by red arrows). Anterior segment ocular coherence tomography image of the (C) right eye and (D) left eye showing hyper-reflective band at DM.

{kind=link}
{kind=link}
Slit lamp image of the (A) right eye and (B) left eye showing sunflower cataract.
Learning points
Ocular manifestations may be the first presenting symptoms of Wilson’s disease which must be recognised to prevent fatal outcomes.
Anterior segment ocular coherence tomography is a useful adjunctive tool for the detection of Kayser-Fleischer rings in suspicious cases.
Footnotes
Contributors SG and PS have contributed to the data acquisition and manuscript preparation. JST has contributed to editing the manuscript. PKM is responsible for the concept, final editing of the manuscript and photographs of the case.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.