Article Text

Statistics from Altmetric.com
Description
A 40-year-old man with a history of cerebral palsy presented to the emergency department with recurrent episodes of vomiting. He had several similar presentations requiring hospital admission over the past 3 years. In 2017, he was admitted for a similar presentation, and CT radiograph demonstrated intestinal obstruction at the proximal jejunal region. He underwent a diagnostic laparoscopy, and a paraduodenal hernia was found. A laparoscopic repair was performed, his symptoms resolved for a short period of time.
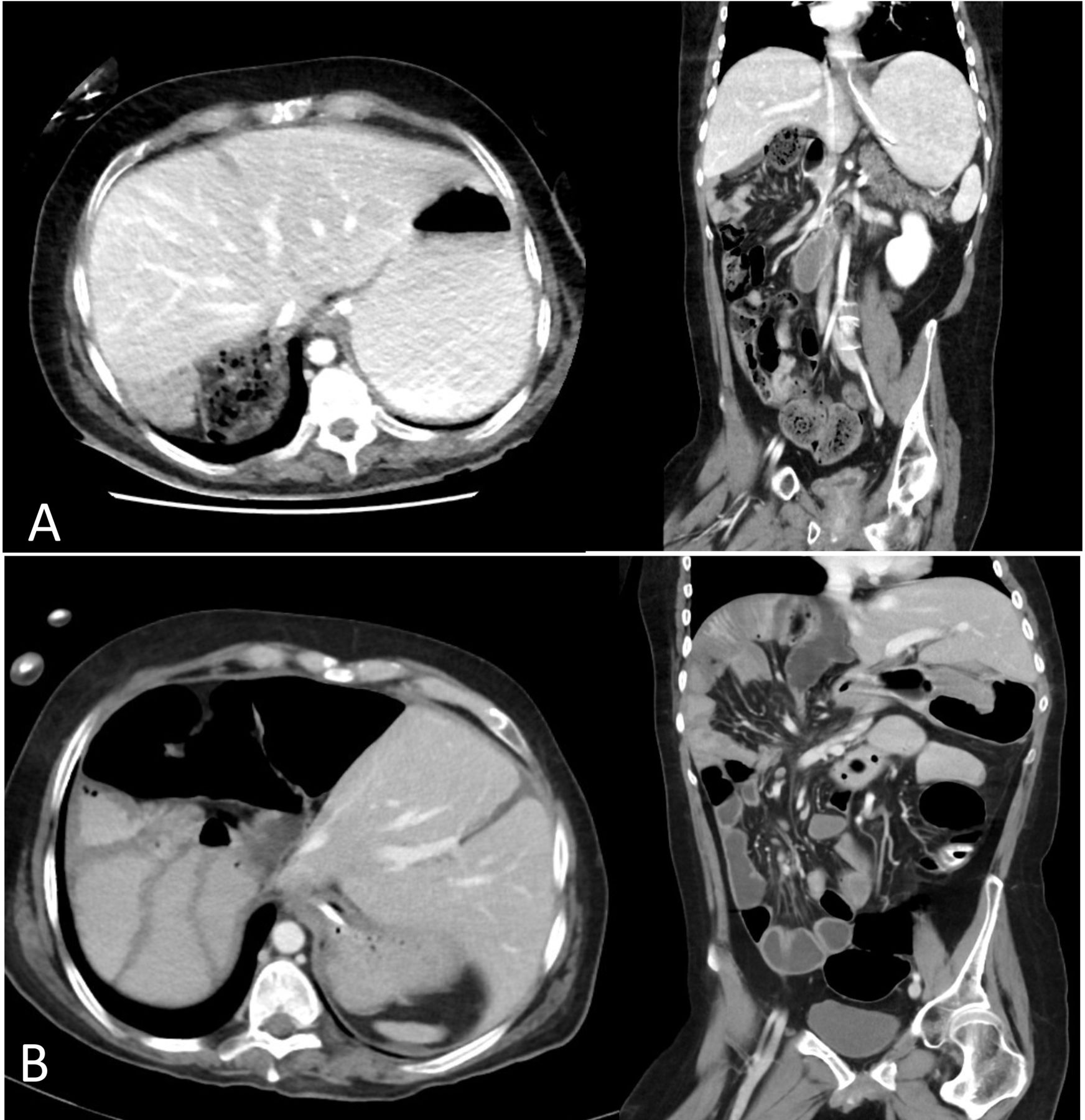
However, after 3 months, his symptoms reoccurred and during multiple presentations a number of CT radiographs were performed. Each CT showed the position of his liver in different locations (figure 1), confirming the diagnosis of a wandering liver.

CT radiographs showing liver in different positions. Liver was in its normal anatomical position on the right side of abdomen (A) compared with a wandering liver which has moved to the left side of the abdomen (B).
Extrinsic compression of duodenum secondary to the wandering liver was suspected. An upper gastrointestinal gastrograffin fluoroscopy with dynamic positioning of the patient was performed. An ultrasound was also performed during the gastrograffin fluoroscopy study to confirm the position of liver during positioning.
When the patient was in right decubitus position, an ultrasound was performed to confirm that the liver was on the right of midline. Contrast was then administered via a nasogastric (NG) tube. The study demonstrated brisk transit. The patient was subsequently repositioned in left decubitus position, and further contrast was administered. This study showed delay in gastric emptying as evidenced by pooling of contrast material in gastric antrum due to extrinsic compression from a wandering liver (figure 2).

{kind=link}
{kind=link}
Gastrograffin fluoroscopy study; patient lying on right side (A) and left side (B).
The patient’s symptoms improved with gastric decompression via NG tube. Oral nutrition was well tolerated, and the patient was discharged home shortly afterwards.
Learning points
Wandering liver or hepatic vagrancy is a rare condition—only 25 reported cases since 1890.1–3
Most reported cases were associated with colonic, predominantly sigmoid, obstruction or volvulus.4
Due to its rarity and non-specific presentation, diagnosis and management of wandering liver remained challenging.2 3 5 6 However, there were two general approaches in treating patients with wandering liver:
Footnotes
Contributors PSB, JF and AB treated the patient. MS was consulted for hepatobiliary surgery opinion.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.