Article Text

Statistics from Altmetric.com
DESCRIPTION
A 35-year-old woman living with HIV presented with progressive wasting syndrome and a slowly growing self-neglected right ankle mass for which she refused to seek medical attention and investigations (biopsy and image studies) for 12 months. There was no previous history of cancer, exposure to chemicals carcinogens or radiation, recreational drug use or alcohol consumption. Examination showed a body mass index of 18 kg/m2 without oral thrush or lymphadenopathy. A large solid fungating dark mass of 26.0×20.0×18.0 cm in size, raised from the right ankle and extended beyond the skin openly. The severely painful tumour contained necrotic soft tissue alternating with haemorrhagic areas (figures 1 and 2). The mass effect on the right lower limb impaired ambulation. The rest of physical examination was normal.
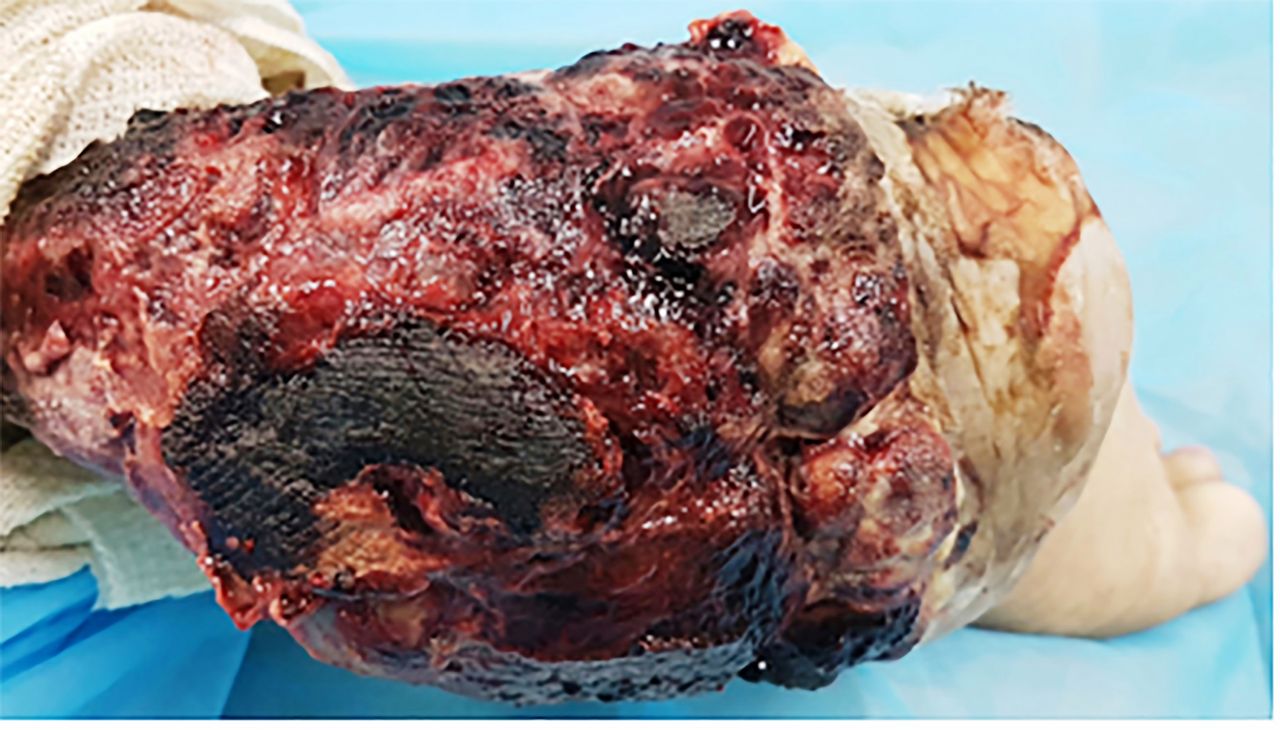
Posterior view image showing a large solid fungating dark mass of 26.0×20.0×18.0 cm in size, arising from the right ankle and extended beyond the skin openly. The mass contains necrotic tissue alternated with soft tissue bleeding areas.

Lateral view image showing the tumour extension beyond the right ankle including the heel and the skin and soft tissue surrounding the heel.
The patient showed suppressed viral loads with good CD4+ T cell counts (table 1). She also received highly active antiretroviral therapy (HAART) (table 2). Extensive investigations for other diseases were negative (table 1). MRI scan of the right ankle showed an irregularly shaped, infiltrating mass, measuring 1.0×3.8×3.1 cm3, located at the medial aspect of the right ankle, and extending into plantar region of the foot along the posterior tibial artery and nerve. This mass demonstrated low T1 signal, mildly high T2 signal and heterogeneous enhancement with intravenously administered Gadolinium. The tendons of foot appeared separate from the lesion. There was no osseous or articular involvement. The bones showed normal MRI signal (figures 3–5). CT scan of the chest revealed multiple soft tissue density bilateral lung nodules, that measured up to 1.0 cm in diameter, suggestive of pulmonary metastasis. Tumour biopsy with histopathology using routine H&E staining and immunohistochemistry supported the diagnosis of synovial sarcoma (figures 6–8). Diagnosed as primary right ankle synovial sarcoma stage IV with metastases to the lung in an adult living with HIV-AIDS, she underwent right above knee amputation, and received palliative therapy. One month later, significant clinical improvement led to discharge her home and subsequent periodic attendant to the oncology and HIV outpatient clinics. Six months later, patient developed metastatic pulmonary haemorrhage and died from this non-aid defining cancer complication despite control of the HIV-AIDS.

MRI scan of right foot and ankle showed a 1.0×3.8×3.1 cm3 irregularly shaped lesion noted at the medial aspect of the right ankle and extending into plantar aspect of the foot, along the posterior tibial artery and nerve. The mass demonstrated high T2 signal on this sagittal fat saturation view.

MRI scan of right foot and ankle shows low T1 signal on this T1-weighted sagittal view.

MRI scan of right foot and ankle with heterogeneous enhancement on IV gadolinium administration on this T1 weighted coronal view. It infiltrates into surrounding subcutaneous fat, without osseous or articular involvement. The tendons of foot appear separated from the lesion.

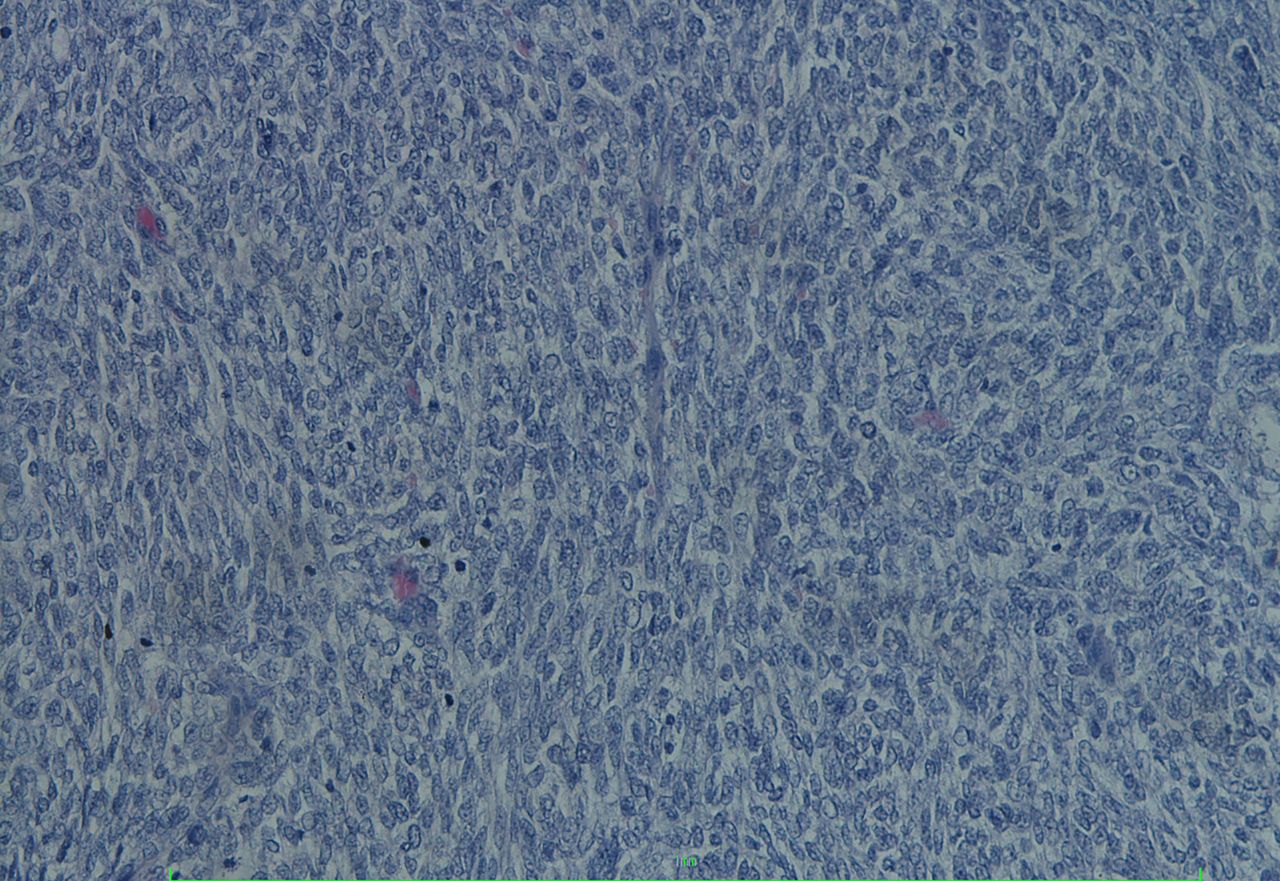
Tumour photomicrography: H&E staining with skin undermined by a monophasic synovial sarcoma with fascicles of spindle shaped cells without epithelial component (20× magnification).

H&E staining showing relatively ovoid uniform cells with occasional mitotic figures (200× magnification).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
On immunohistochemistry, the tumour cells showed expression of Bcl-2 with strong staining and diffuse positive (4+) (40× magnification).
Medical investigations
Medical treatment
In 2015, there were 36.7 million people living with HIV-AIDS worldwide but the global coverage of HAART reached only 46%. Several long-term studies have indicated an increased risk for the development of a multitude of non-AIDS-defining cancers in HIV-AIDS patients such as non-Hodgkin’s lymphomas, Kaposi sarcoma and cervical cancer. Very few reports, however, exist regarding the occurrence of non-AIDS-defining sarcomas in the extremities.1 The literature rarely mention the occurrence of bone and soft tissue tumours and also fail to describe the histological nature and site of these malignancies. Conventional synovial sarcoma among those patients with ages between 30 and 60 years is extremely rare. We have not found a previous publication regarding the occurrence of synovial sarcoma among people living with HIV.1 The pathogenesis of many malignancies associated with HIV infection is not yet completely understood, but it may involve concomitant viral or other microbial infections with direct carcinogenic actions or indirectly through immunosuppression.2 3
Learning points
Synovial sarcoma of the ankle is an extremely rare and aggressive form of cancer but is perhaps unique as a concurrent malignancy among adults living with HIV-AIDS.
Several comprehensive long-term follow-up studies rarely mention the occurrence of bone and soft tissue tumours among HIV-AIDS patients and also fail to describe the histological nature and site of these malignancies.
The relationship of HIV-AIDS with osteosarcoma or sarcoma or synovial sarcoma remains uncertain
The immunological basis of the development of malignancies in HIV-infected individuals is not yet completely understood. The pathogenesis of HIV inducing malignancy may involve direct virus carcinogenic actions or indirectly through immunosuppression.
A greater index of suspicion is required in HIV patients presenting with unexplained bone and joint pain or swelling. Appropriate radiological investigation and timely referral to a specialised orthopaedic and oncology unit are recommended.
Footnotes
Contributors Conception and design, acquisition of data or analysis and interpretation of data was performed by AJR. Drafting the article or revising it critically for important intellectual content was done by AJR, WG, KR and FR. Final approval of the version published was done by all authors. All authors agree to be accountable for the article and to ensure that all questions regarding the accuracy or integrity of the article are investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.