Article Text

Statistics from Altmetric.com
Description
A 19-year-old man presented with painful lesions all over the body for last 25 days. Cutaneous examination revealed multiple fluid-filled bullae and tender ulcers of varying size with undermined violaceous borders (figure 1A–D) distributed over face, bilateral upper, lower limbs and trunk. On per abdomen examination, spleen was palpable 4 cm below the left costal margin. Histopathological examination from the blister on the left lower leg revealed subepidermal blister. In addition, there was dense neutrophilic infiltrate along with few lymphocytes mainly within the dermis (figure 2A, B). Fungal, bacterial and mycobacterial cultures were sterile. His blood tests revealed a white blood cell count of 2.19x102/L with 95% neutrophils and 4% lymphocytes, haemoglobin of 0.72g/L and platelets of 1.2x101/L. Blood urea levels were 260 mg/dL and serum creatinine was 2.8 mg/dL. Antinuclear antibody, rheumatoid factor, anticardiolipin antibody, myeloperoxidase and antineutrophil cytoplasmic antibody titre were negative. ECG revealed no significant findings. Patient could not be evaluated further as he died within a week of admission.

(A)Dorsal aspect of the hand with variable-sized fluid-filled bullae and superficial ulceration at places. (B) Single intact tense bulla of size 2.5 cm approximately present over the left nasal ala and a crusted erosion present over the right nasal ala. (C) Single ulcer of size 2×3 cm with undermined edges and surrounded by peripheral erythema present over the left lower limb. (D) Two well-defined oval ulcers of size ranging from 3–4^2–3 cm with regular margins, undermined edges and floor covered with whitish slough present over the groin.

{kind=link}
{kind=link}
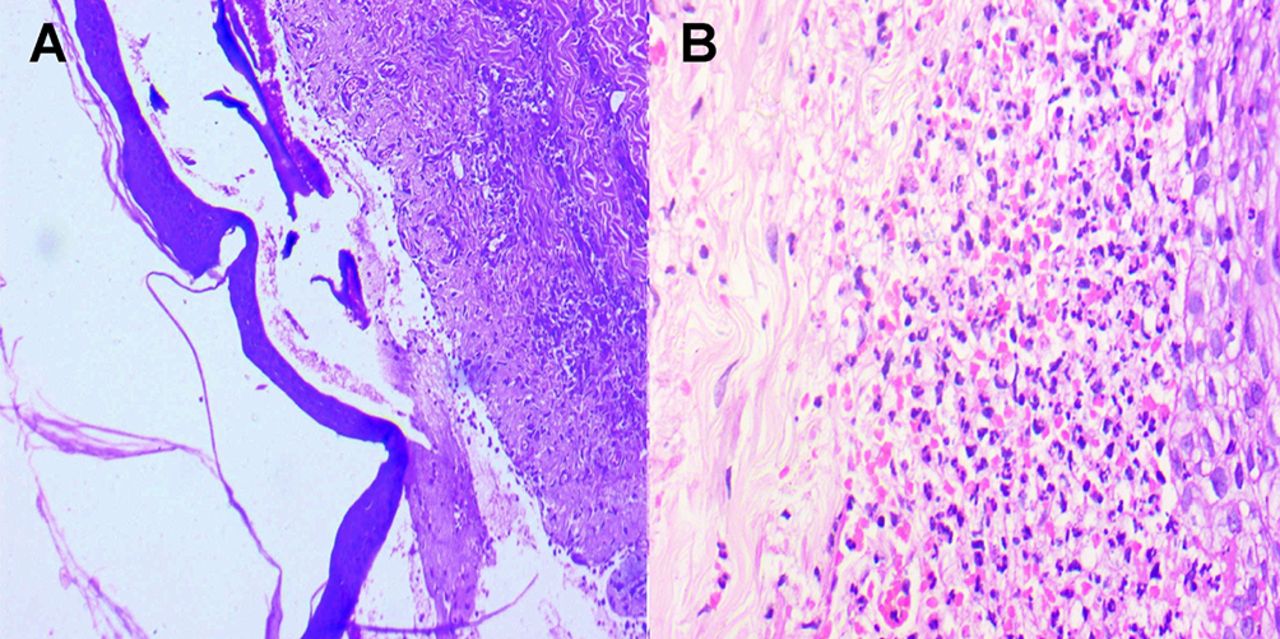
(A) Skin biopsy from bulla over the left lower limb showing subepidermal bulla with neutrophils (H&E stain; ×40) (B) Dense infiltrate of neutrophils with few lymphocytes present in the dermis (H&E; ×40).
Pyoderma gangrenosum (PG) is a sterile neutrophilic dermatosis of unknown aetiology. Commonly affected age group is 40–60 years. Ulcerative, bullous, pustular and vegetative forms are the different clinical variants. Bullous PG is rare and was first described by Perry and Winkelmann in 1972.1
Classic PG is characterised by deep ulcers with undermined borders while in bullous variant there are superficial ulcers. Upper body is commonly involved in the bullous variant while lower extremity involvement is common in classic PG.1 Lymphoproliferative diseases, inflammatory bowel disease, rheumatoid arthritis and so on are frequently associated with this subtype. Haematological malignancy is found in about 70% of cases. Thirty eight cases of bullous PG were reviewed by Sakiyama et al and it was found that the most commonly associated haematological disorders were acute myeloblastic leukaemia (44.7%) and chronic myelogenous leukaemia (10.5%).2
Diagnosis is determined on the basis of clinical features and evolution of the lesion (rapid progression). Histopathological findings are only supportive and depend on the site and stage of the lesion. Biopsy from the centre of the ulcer shows massive neutrophilic infiltrate in the absence of vasculitis and granuloma formation and the one done from periphery of the lesion will have lymphocytic infiltrate predominantly. In addition to the above findings, there can be epidermal necrosis with subepidermal blister in cases of bullous PG.1
Vasculitis (Wegener’s granulomatosis, livedoid vasculitis, polyarteritis nodosa and so on), infections (deep fungal, bacterial), malignancies (lymphomas, leukaemia), neutrophilic dermatoses (atypical Sweet’s syndrome, Behcet’s disease) and drug reactions are some of the important differentials.1 Caughman et al 3 suggested that bullous PG and atypical Sweet’s syndrome represent two different ends of the same spectrum of disorders.
Treatment of the underlying disorder can help in early healing of the ulcer. Systemic corticosteroids are the first-line treatment while drugs like cyclosporine, methotrexate, azathioprine, cyclophosphamide, sulphasalazine, dapsone, clofazimine and rifampicin can also be given.1 Pathergy phenomenon can be seen in this dermatosis hence surgical intervention should be avoided.
Learning points
Bullous pyoderma gangrenosum is mostly associated with haematological abnormality.
Upper extremity is the the most common site involved and is characterised by superficial ulcers as compared with the classical variant.
Subepidermal bulla can be seen on histopathology in addition to the tissue neutrophilia.
Footnotes
Contributors Conception and design, acquisition of data or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content: SS, SP and AS. Final approval of the version published; agreement to be accountable for the article and to ensure that all questions regarding the accuracy or integrity of the article are investigated and resolved: SS and SP.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Parental/guardian consent obtained.