Article Text

Abstract
Schistosomiasis is infrequently seen in the UK, but remains an important cause of haematuria in endemic areas. It may also be complicated by systemic illness, and can affect multiple organs, including the bladder, liver and lungs. We discuss a case of haematuria associated with lower abdominal discomfort and dry cough/wheeze in a returning traveller diagnosed as pulmonary and urinary schistosomiasis, caused by Schistosomahaematobium. This case was particularly notable for the radiological findings seen on CT scan of the chest (figure 2A,B), as well as the characteristic sago nodules discovered within the bladder. It is also unusual to see pulmonary schistosomiasis associated with S. haematobium, an organism more typically characterised by bladder involvement. It is important to consider schistosomiasis and its complications, while rare in the western world, it remains an important differential diagnosis in at-risk groups with considerable morbidity if untreated.
- infections
- tropical medicine (infectious disease)
- urology
- respiratory medicine
- infectious diseases
Statistics from Altmetric.com
Background
Pulmonary disease is rarely seen in Schistosoma haematobium, and is more commonly associated with Schistosoma mansoni.1 Chest symptoms may be seen in acute infection as part of ‘Katayama fever’, a flu-like illness seen within 2 months of exposure. This syndrome is caused by the release of eggs and the associated rapid rise in antigen burden. Acute pulmonary schistosomiasis tends to be characterised by dry cough and wheeze.1
The chest symptoms our patient experienced were more chronic, the pathology in these cases is a granulomatous pulmonary endarteritis (which if untreated progresses to fibrosis with pulmonary hypertension and cor pulmonale). Chronic pulmonary involvement is more likely to present as dyspnoea, although in our case cough and wheeze remained a feature.1
Case presentation
A 25-year-old man presented to his general practitioner (GP) with two episodes of lower abdominal pain and haematuria 3 months apart associated with a feeling of irritation in the bladder/penis. He also reported a sensation of incomplete emptying and frequency. Urine dip and blood tests done by the GP were unremarkable, as were nucleic acid amplification tests for gonorrhoea and chlamydia. He had previously been fit and well, with no past urological history, and a medical history notable only for recent travel to Ghana, where he had been swimming in Lake Volta, he denied any other travel history and remained asymptomatic throughout his time in Ghana (no itching or dermatological symptoms of note).
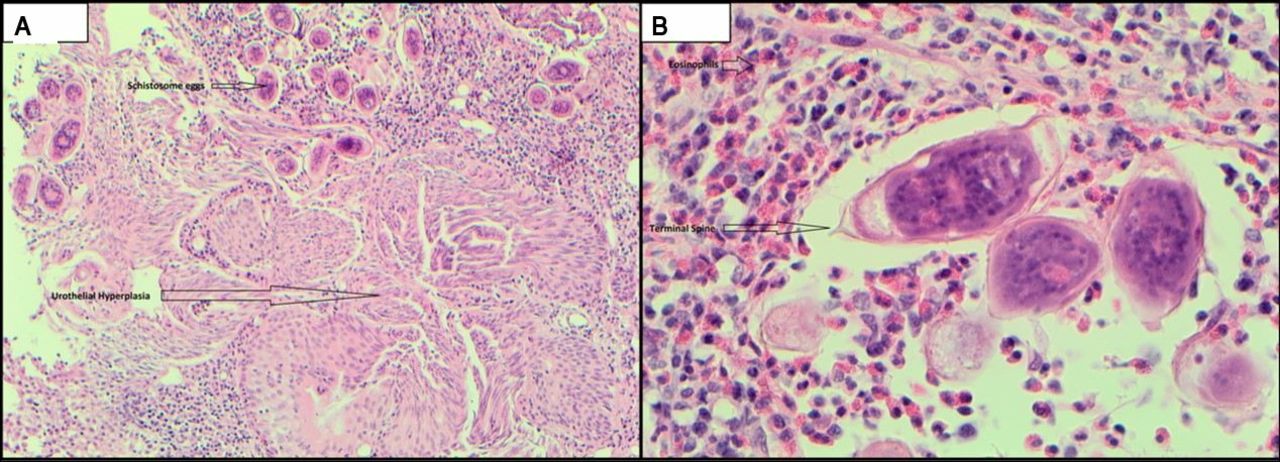
In light of his haematuria, he was referred to urology for further investigation. An elective flexible cystoscopy was performed, showing an area of ‘abnormal mucosa’ at the trigone of the bladder. To further investigate the lesion a transurethral resection of bladder tumour (TURBT) was planned, at that time the abnormal mucosa was again identified and biopsied; note was also made of yellow nodules seen at the base of the bladder, suspicious for sago nodules associated with schistosomiasis. Samples of the bladder wall were sent for histology (figure 1A,B) which showed:

(A) is a wide view at ×10 magnification showing histology of affected bladder tissue showing urothelial hyperplasia and schistosome eggs. Urothelial hyperplasia describes a thickening of the urothelium in the absence of any structural or cytological atypia. Granulomatous inflammation is also a typical feature. (B) shows schistosome egg seen at ×40 magnification. The schistosome eggs are typically oval (~140×50 μm) with a sharp terminal spine, which can be used to distinguish between Schistosoma haematobium and other common Schistosoma species (S. japonicum and S. mansoni have lateral spines).
Granulomas (both necrotising and non-necrotising).
Urothelial hyperplasia with oedema.
Chronic active inflammation.
Numerous eosinophils centred around schistosome eggs with a distinctive terminal spine characteristic of S. haematobium.2
At the time of the TURBT, the patient also made a comment regarding a chronic cough and wheeze, which was particularly noticeable in the evenings. The cough was of unclear duration but based on the appearance of the bladder and history suspicious for schistosomiasis, a CT chest was requested as an outpatient. This CT showed multiple pulmonary nodules (figure 2A and B), some of which were associated with ground-glass haloes, some sub solid. Although S. haematobium seldom affects the lungs1 3, these findings are typically seen with pulmonary schistosomiasis1 and in this context are highly suspicious for lung involvement.

{kind=link}
{kind=link}
High-resolution CT images showing (A) solid and (B) subsolid, non-cavitating pulmonary nodules within the right lung. A typical ground-glass halo is seen surrounding the solid central component of the nodule in (B), which represents haemorrhage. These findings are highly suspicious for pulmonary schistosomiasis given the patient’s history and bladder histology.
At the time of histological confirmation of diagnosis, the patient was being treated in the hospital for haematuria with clots. These symptoms had largely settled with hydration before antischistosomal treatment could be initiated with two doses of praziquantel, which produced a rapid and lasting resolution of both his chest and urinary symptoms.
Investigations
The patient’s blood tests were persistently normal throughout, with no change in renal function or eosinophilia/leucocytosis.
An ultrasound of the renal tract was entirely normal, as was a CT urogram.
Differential diagnosis
Persistent visible haematuria in the absence of infection or other clear causes is clearly of concern. Patients with this presentation should be investigated with cystoscopy and CT urogram to investigate for bladder cancer or renal pathology, respectively.
The history remains important, as it informs our interpretation of what we see. If no travel history is taken, the abnormal mucosa seen within the bladder could be mistaken for a consequence of bacterial infection and treated inappropriately.
Vasculitides and autoimmune conditions, such as granulomatosis with polyangiitis and Goodpasture’s, can also present with respiratory symptoms and haematuria. Similar nodules may also be seen on CT but we would expect derangement in renal function to be evident on the blood tests.
Treatment
Two doses of praziquantel (two doses of 20 mg/kg 8 hours apart).
Outcome and follow-up
The patient improved rapidly after treatment, with significant improvement of urinary as well as respiratory symptoms.
Discussion
Schistosomiasis is a parasitic infection, primarily caused by three species of flatworm4:
S. mansoni, seen in Africa and South America, typically causing intestinal/hepatic disease.
S. japonicum, seen in East Asia, typically causing intestinal/hepatic disease.
S. haematobium, seen in Africa and the Middle East, typically causing genitourinary disease.
The prevalence is high within Sub-Saharan Africa, and an estimated 200 million people are infected worldwide.4 Despite these numbers, schistosomiasis is rarely seen in the western world, although prevalence has increased in recent years with the increasing popularity of adventure/charity tourism, particularly the trend of travelling to poorly developed rural areas.5
The disease is transmitted by defaecation/urination into fresh water, releasing eggs into the environment, which hatch into miracidia, these infect freshwater snails act as intermediate hosts for several life-cycle stages before the pathogens leave the snail as cercariae. These cercariae are able to infect human hosts through exposed skin, often causing a localised itch, before migrating into the circulation as schistosomulae to reach the liver where they develop into adult worms. The adult worms then migrate into the bloodstream once more, settling in the venules of the bladder/gastrointestinal tract depending on the species. Once there, they release eggs into the urine/faeces, which return to the environment.4
Untreated, schistosomiasis can lead to significant morbidity, including iron deficiency anaemia, intestinal strictures, portal hypertension, cor pulmonale and bladder cancer. However, treatment is simple where there is access to medicines, and public health measures have eliminated the disease in several countries where it was previously widespread.6
Learning points
Schistosomiasis is a rare but increasingly important cause of haematuria, particularly in travellers.
Symptoms of schistosomiasis are often mild, and routine tests frequently show no abnormality.
Pulmonary schistosomiasis is relatively uncommon but associated with significant morbidity including cor pulmonale.
Treatment of schistosomiasis is easy once the diagnosis is made, controlling the spread of disease in the community is more difficult but possible.
Footnotes
Contributors Case report drafted and images obtained by JM. Review of draft and revisions as recommended by SH, also provided help in the interpretation of CT imaging. Final approval is given by both authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.