Article Text

Statistics from Altmetric.com
Description
A 63-year-old woman presents to the medical receiving unit with a 2-month history of violaceous haemorrhagic nodules on her right lower leg on the background of 10-year history of chronic lymphoedema (figure 1). She had a complex medical history including previous deep venous thrombosis (DVT) of the right leg, atrial fibrillation, hypertension, chronic kidney disease, ischaemic heart disease, non-alcohol related fatty liver disease and a progressive neurodegenerative disorder. The worsening spasticity in her lower legs ultimately reduced her mobility and she was subsequently a wheelchair user. The DVT, recurrent cellulitis and immobility/dependency led to the development of chronic lymphoedema.

Violaceous nodules on the shin with evidence of skin changes consistent with chronic lymphoedema of the right lower leg.
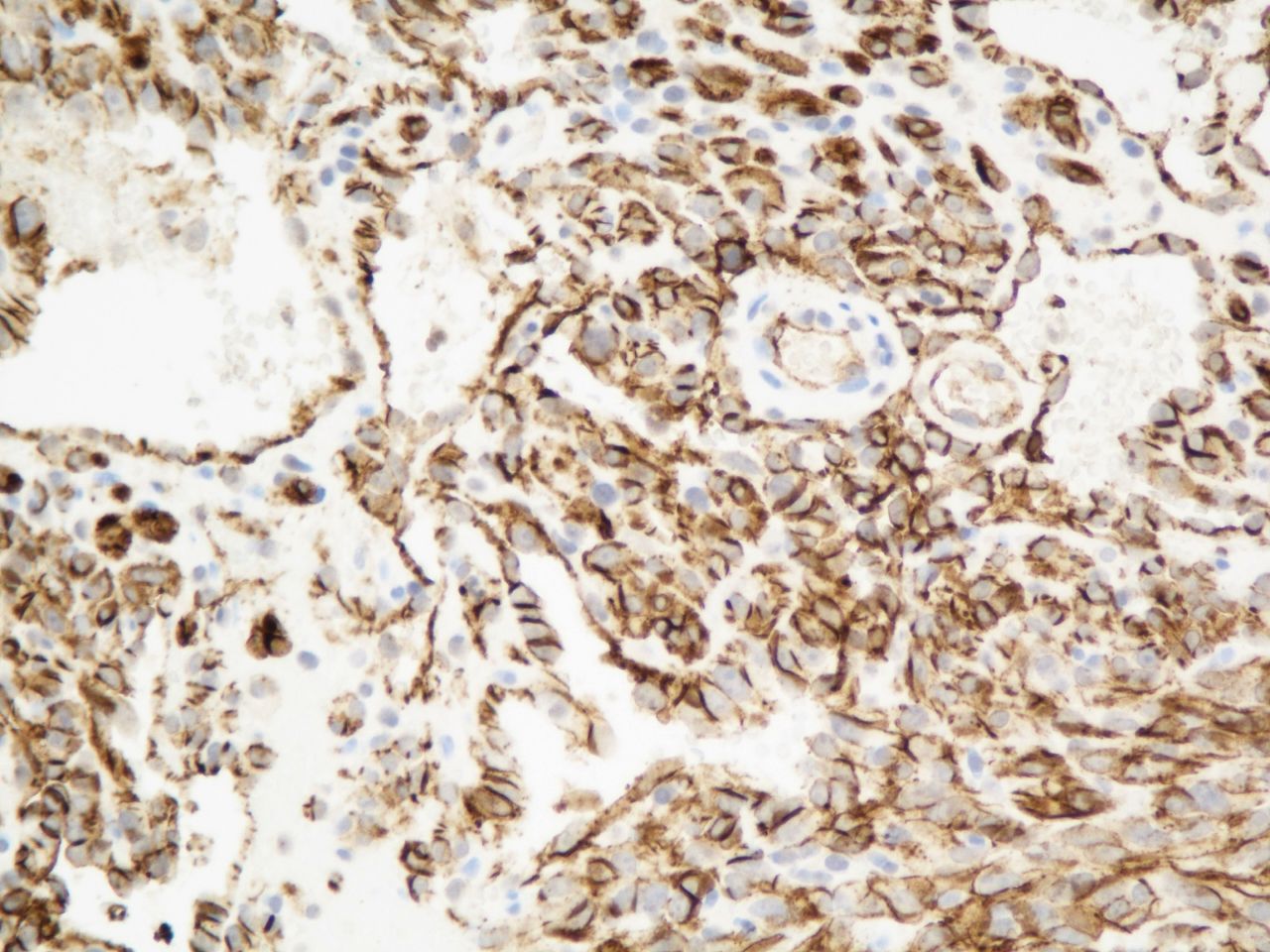
A skin biopsy confirmed cutaneous angiosarcoma (figures 2 and 3). Staging CT of the chest, abdomen and pelvis excluded metastatic disease. An MRI scan did not identify any discrete enhancing lesions in the subcutaneous tissues of the right leg. She subsequently had a right transfemoral amputation under the care of the sarcoma specialists following discussion at the National Sarcoma multidisciplinary team meeting. Histology confirmed that clear margins were achieved. She has since recovered without any significant complications and is under the care of the surgical and oncology teams for monitoring for disease recurrence or metastatic disease every 3 months. Adjuvant therapy such as chemotherapy was not warranted with clear surgical margins and in the absence of metastases.

Microscopy showed a high-grade malignant spindle cell tumour with vascular channel formation and red cell extravasation.

{kind=link}
{kind=link}
{kind=link}
The tumour cells were positive with the immuno-histochemical marker CD31, confirming angiosarcoma.
Angiosarcoma is a malignant neoplasm of endothelium that can rarely occur in the context of chronic lymphoedema, known as Stewart-Treves syndrome. This entity, first described in 1948, has historically been associated with post-mastectomy and axillary node dissection following breast cancer diagnosis and therefore usually presents in the upper limbs. It can also be broadly applied to tumours occurring in the lower extremities in patients with primary or secondary chronic lymphoedema. The duration of the lymphoedema prior to appearance of the tumour can range anywhere between 1 and 26 years.1 The pathophysiology is still unknown and it is postulated that lymphostasis induces local immunodeficiency and poor immunosurveillance which subsequently promotes vascular oncogenesis.2
Stewart-Treves syndrome initially presents with subcutaneous violaceous nodules or eschars which can then progress and coalesce to form indurated plaques with evidence of pitting oedema. Histopathological and immuno-histochemical studies are essential for diagnosis. There is no consensus on the optimal management of angiosarcoma in Stewart-Treves syndrome, but some major sarcoma centres advocate a radical amputation involving forequarter or hindquarter amputation.3 Chemotherapy with paclitaxel has been used in a palliative setting in patients with inoperable disease.
This tumour is highly aggressive and prone to metastasis. The overall prognosis is poor with a median survival of 2.5 years.3 Therefore, it is important for clinicians to recognise this rare complication of chronic lymphoedema in order to expedite appropriate investigations and treatment. A multidisciplinary approach is vital in the care of these patients. In summary, we present a case of a 63-year-old woman with Stewart-Treves syndrome, a rare cutaneous angiosarcoma on the background of chronic lymphoedema.
Learning points
Cutaneous angiosarcoma is a malignant vascular neoplasm for which there are three main variants: idiopathic, post-radiation and in chronic lymphoedema of the upper limb typically post-mastectomy (Stewart-Treves syndrome).
Stewart-Treves syndrome presents as bruise-like patches/plaques, violaceous nodules or ulcerating lesions on the background of lymphoedema. Skin biopsy is imperative to confirm diagnosis.
The prognosis is poor and therefore early recognition is essential to prevent delay in diagnosis and management.
Footnotes
Patient consent for publication Obtained.
Contributors All authors were involved with the patient’s care, contributed to the writing of this article and approved the submitted article. AR was responsible for acquisition of clinical data, literature review, conception and article writing. MP, SL and GW revised it critically for important intellectual content and all authors approved the final version/submitted article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.