Article Text

Abstract
Certain interventional pulmonology procedures such as the placement of a tracheal stent or resection of stenosing tracheal tumours require rigid bronchoscopy under general anaesthesia. Unlike an endotracheal tube with a cuff, the rigid bronchoscope only partially protects the airway from bronchoaspiration. For this reason, this procedure is performed on an elective basis in fasted patients. We describe the case of a 60-year-old man with acute respiratory distress requiring emergent rigid bronchoscopy following distal migration of a tracheal stent. One hour before the procedure, the patient had eaten a full meal. Gastric emptying was accelerated by perfusion of intravenous erythromycin and verified by endoscopy with a small diameter gastric endoscope under local anaesthesia. This 1 min procedure was very well tolerated by the patient and allowed to verify with certainty that the stomach was empty. The urgent rigid bronchoscopy for stent retrieval could then be performed safely without any risk of bronchoaspiration.
- anaesthesia
- gastrointestinal system
- emergency medicine
- endoscopy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Gastric inhalation is one of the most feared complications in anaesthesia and can lead to acute respiratory distress syndrome1 with up to 40% mortality.2 Its incidence varies between one in 978 and one in 7103 general anaesthetics,3 4 but it can increase up to 10-fold in the emergency setting.5 To reduce the risk of bronchoaspiration, patients presenting for elective surgery are fasted 6 hours for solid food and 2 hours for clear liquids,6 although these deadlines may not be respected in emergency situations. In addition, the presence of stress, pain and morphine administration usually delay gastric emptying.7–9 In 2015, the efficacy of erythromycin, a macrolide antibiotic and motilin receptor agonist, was shown for gastric emptying in patients undergoing general anaesthesia for emergency surgery.10
Gastroscopy is considered as the gold standard to evaluate the type and volume of gastric content and to measure its acidity.10 However, due to the large diameter (9–11 mm) of the endoscopes, it is considered as uncomfortable in awake patients presenting for general anaesthesia in an emergency setting. The preferred method for the estimation of the volume of gastric content preoperatively is ultrasound, but it has the disadvantage that incomplete gastric emptying cannot be ruled out with certainty11 12 and an examination may be impossible for various reasons, such as air in the stomach, obesity or operator inexperience.11 Recently, new small diameter gastric endoscopes (4.8 mm) are available and their introduction through the nose under local anaesthesia is very well tolerated by patients, often without any sedation. We propose to use this technique in emergency patients to verify gastric content before general anaesthesia instead of gastric ultrasound.
Case presentation
We report a case of a 60-year-old man with a smoking history of 25 pack years stopped in 2001, high blood pressure, hypercholesterolaemia and depression. In 2011, the patient underwent curative medium and lower right bilobectomy for a stage IB squamous cell lung carcinoma, followed by radiotherapy and chemotherapy.
In October 2017, cancer recurrence was diagnosed with bilateral pulmonary and tracheal metastasis. One month later, the patient developed dyspnoea with inspiratory and expiratory stridor in the context of a mixed tracheal mass (intrinsic and extrinsic) visualised by a computer tomography scan of the chest (figure 1). The patient was scheduled for rigid bronchoscopy under general anaesthesia and fasted 6 hours for solid food and 2 hours for clear liquids. The examination confirmed the presence of a mixed tumour of the proximal trachea located 40 mm from the vocal cords with a critical narrowing of its lumen over 40 mm in length (figure 2). After partial resection of the intrinsic component of the tracheal metastasis using a bronchoscope and YAP (Yttrium-Aluminum-Perovskite) laser (Lokki Lis Laser, Bryan, Woburn, USA), an 18×50 mm self-expanding, fully covered metal stent was placed to contain the residual extrinsic compression. The resection was only partial to maintain the stent in place. The procedure was performed without complications with immediate resolution of dyspnoea. Radiography of the thorax confirmed the correct placement of the tracheal stent (figure 3).

Chest tomography scan on the mediastinal window shows tracheal stenosis due to the mixed tracheal mass. Yellow arrow shows stenosis on CT scan.

Mixed tumour of the proximal trachea, located 40 mm from the vocal cords, producing a critical narrowing of its lumen over 40 mm in length.

Radiography of the thorax confirms correct placement of the tracheal stent. Yellow arrow shows the positioning of the stent.
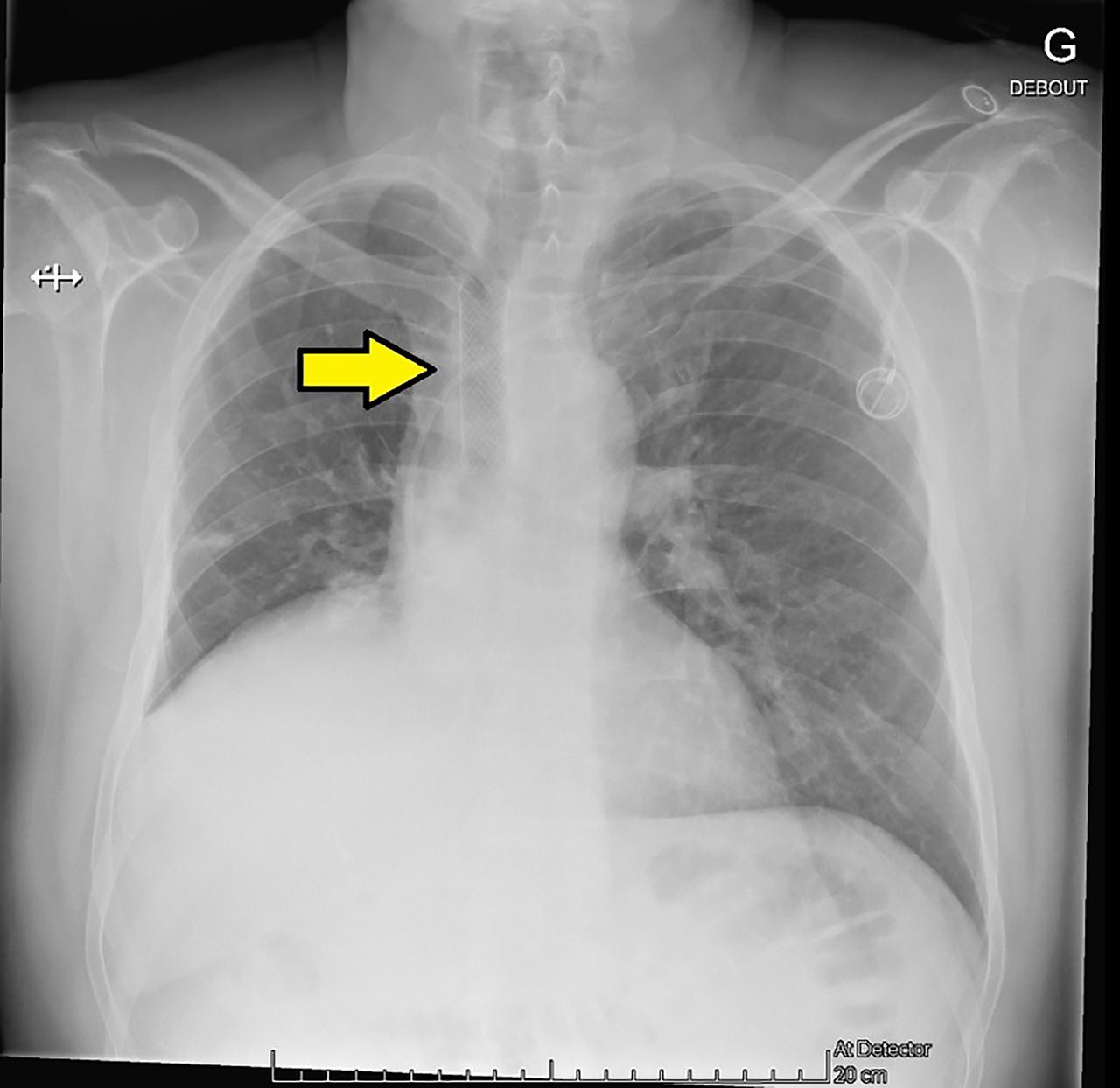
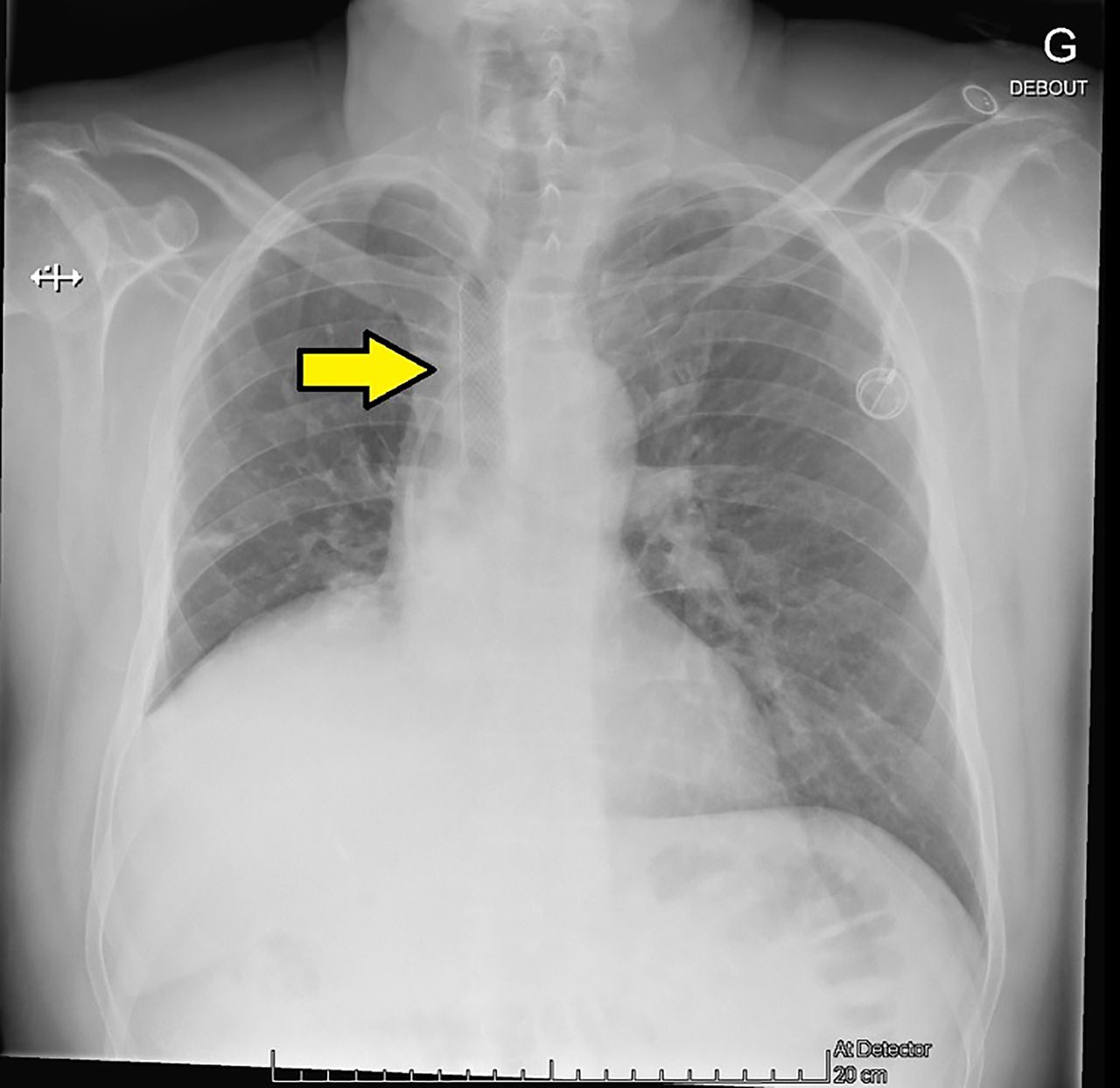
On postoperative day 1, the patient experienced severe acute dyspnoea (grade 4 of the modified Medical Research Council dyspnoea scale)13 at rest with chest discomfort after a period of intense coughing. Oxygen saturation was 94% at ambient air. Chest X-ray confirmed migration of the tracheal stent requiring emergent rigid bronchoscopy for its retrieval (figure 4). The dyspnoea was attributed to the extrinsic component of stenosis and the irritation caused by the displaced stent. As he had eaten a full meal in the previous hour, 250 mg (3 mg/kg) of intravenous erythromycin was administered to accelerate gastric emptying. One hour later, a senior gastroenterologist performed gastric nasofibroscopy under local anaesthesia using a nasofibroscope (Olympus Europa SE & Co, Hamburg, Germany) with an external diameter of 4.8 mm. The patient was positioned on the bronchoscopy table in the operating room with the head slightly up. Intranasal and oral local anaesthesia was administered using a 10% lidocaine spray. The procedure was of very short duration (50 s), very well tolerated and confirmed the complete emptying of the stomach (video 1). This allowed the general anaesthesia for rigid bronchoscopy to be performed safely without any risk of bronchoaspiration. Bronchoscopy revealed a distal migration of the tracheal stent, which was removed with forceps. Additional resection of the tumorous mass was performed with the YAP laser, without the need to place a new stent as the tracheal calibre was satisfactory.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Radiography of the thorax confirms migration of the tracheal stent. Yellow arrow shows the positioning of the stent.
Endoscopic control of gastric emptying before anaesthesia induction with patient awake.
One month later, another emergency bronchoscopy was necessary due to an aggravation of dyspnoea in the context of tumour progression. As the patient was not fasting, he received intravenous erythromycin again followed by gastric nasofibroscopy under local anaesthetic, which showed complete gastric emptying. Bronchoscopy confirmed severe tracheal stenosis with a residual lumen of approximately 20% of the normal lumen, which required the implantation of a new 18×60 mm silicone tracheal stent with excellent immediate results. The procedure was uneventful.
Outcome and follow-up
Unfortunately, the patient died 6 months later due to tumour progression.
Discussion
To our knowledge, this is the first case report of the endoscopic control of gastric content with a small diameter nasogastric endoscope under local anaesthetic in an awake patient scheduled for general anaesthesia for rigid bronchoscopy in an emergency setting. The procedure was well tolerated and lasted only for 50 s.
We were very concerned as to whether the patient’s stomach was empty before inducing general anaesthesia as he had eaten a full meal shortly before his coughing attack and displacement of the tracheal stent. The slightest amount of gastric content aspirated to the lungs could have been fatal in this patient with advanced lung cancer. Gastric emptying was accelerated by intravenous erythromycin 1 hour before the procedure. Erythromycin causes antral contractions,14 increases the tone of the lower sphincter of the oesophagus15 and allows gastric emptying through its pro-kinetic effects.10 16 However, it does not guarantee complete emptying in all patients.10 Liquids are easily emptied, whereas gastric emptying half-times after a solid meal range between 4017 and 160 min.16 For this reason, we administered erythromycin 1 hour prior to the procedure.
In our particular context where a general anaesthetic had to be performed without securing the airway with an orotracheal tube with a cuff, it was essential to be sure of the emptiness of the stomach in order to avoid the risk of inhalation18 as the rigid bronchoscope only partially protects the upper airways. The only examination that can confirm that the stomach is empty with certainty is gastroscopy. However, since the diameter of classic gastric endoscopes is relatively large, this examination is considered as uncomfortable in an awake patient. Fortunately, new gastric endoscopes with smaller diameters are now available. Introduced through the nose after intranasal and oral local anaesthesia, this examination is well tolerated in a patient psychologically prepared for the procedure. In our patient, we were able to confirm complete emptiness of the stomach in our patient and proceed immediately with a general anaesthesia. This examination would also have allowed to aspirate residual gastric content if only fluid had been present or to visually estimate the volume of solid or mixed gastric content. In the case of a full stomach, we would have given either a supplemental dose of intravenous erythromycin or changed our strategy for rapid sequence intubation with a large diameter endotracheal tube with balloon and retrieval of the stent without concomitant visualisation of the trachea. We performed this examination twice in this patient on two different occasions, which demonstrates the reproducibility of our procedure.
The most frequent alternative for the preoperative assessment of gastric content in the emergency setting is gastric ultrasound, which requires experienced and skilled operators. The antral cross-sectional surface area is measured and correlated with the gastric volume, a formula described by Bolondi et al.19 However, this examination does not allow to affirm 100% that the stomach is empty, especially in the case of obesity or the presence of air in the stomach.11 Performing nasofibroscopy is simple and of shorter duration than gastric ultrasound, which requires several measurements11 12 and has the disadvantage of providing operator-dependent results. Although more invasive than a simple stomach ultrasound, nasofibroscopy performed in a cooperating patient is less invasive than the introduction of a nasogastric tube as it is done under visual control. We propose to consider gastric nasofibroscopy as part of the anaesthesiologist’s armamentarium as s/he is used to fibroscopy during fibre-optic intubation or when checking the correct positioning of double lumen tubes. Importantly, this ultimate control of gastric emptying allows to optimise the anaesthetic strategy and to contribute to patient safety.
Learning points
Small diameter nasogastric endoscopy under local anaesthetic is a rapid, well-tolerated procedure to assess gastric content in patients presenting for emergency tracheal intubation.
Anaesthetists should be aware that this procedure is a valid alternative to gastric ultrasound and allows to determine the presence or absence of gastric content with absolute certainty and to adapt the anaesthetic strategy accordingly.
When only gastric liquids are present, they can be aspirated and the stomach can be emptied by using this procedure. The volume of solid or mixed gastric content can be estimated and the effect of intravenous erythromycin verified.
We consider that it would be beneficial that gastroenterologists help to raise awareness of this alternative to gastric ultrasound. Only experienced endoscopists should perform this procedure.
Anaesthetists may perform small diameter gastric endoscopy following appropriate training by experienced endoscopists.
Acknowledgments
We thank Rosemary Sudan for editorial assistance.
References
Footnotes
Contributors SN drafted the first version of the manuscript and received informed consent from the patient. J-LF is the gastroenterologist who performed the endoscopic control. JP is the pulmonologist of the patient who performed the bronchoscopy. SN and CC are the anaesthesiologists of the patient. CC filmed the endoscopic control and revised the manuscript. J-LF and JP critically revised the manuscript. All authors read and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.