Article Text

Abstract
A 69-year-old Japanese woman with a post-hysterectomy status came to our primary care clinic. She presented with vaginal bleeding for the past 3 days which had developed after defecation. There was a palpable mass measuring approximately 2 cm on pelvic exam; however, heavy bleeding prevented in-depth observation. CT and MRI scans revealed that the mass was inside the urethral meatus and not in the vagina. She underwent surgical resection of the urethral tumour, and the pathological report showed no malignancy. A final diagnosis of urethral caruncle was made. Vaginal bleeding is commonly encountered in the primary care practice and is usually attributed to gynaecological diseases. However, patients and physicians may falsely regard urinary or gastrointestinal tract bleeding as one involving the genital tract. We present a case wherein vaginal bleeding was initially considered but was later identified to be due to a urethral caruncle.
- vulvovaginal disorders
- sexual health
- haematuria
- urology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Genital tract bleeding can be falsely considered when patients are bleeding from sources outside of the genital tract, such as the urethra, bladder, anus, rectum, sigmoid colon or large intestine. Moreover, causes of bleeding can be due to systemic diseases, including bleeding disorders, liver and renal diseases or benign or malignant neoplasms. Diagnostic errors in the source of bleeding may lead to inappropriate consultation, inappropriate testing and prolonged symptoms. Thus, it is important to accurately locate the bleeding source through direct observation so that appropriate specialist consultation can be made in a timely manner.
Case presentation
A 69-year-old woman developed abdominal discomfort 3 days prior to presentation, when she noticed a copious amount of bleeding in a toilet after defecation. The bleeding continued regardless of defecation and urination. She was not experiencing fever, nausea, appetite changes, hematochezia, haematuria, diarrhoea, dysuria, abdominal pain or recent medication changes. Her previous medical history included a total hysterectomy with unilateral salpingo-oophorectomy for stage 1 cervical cancer at the age of 42. Her current medications did not include anticoagulants or antiplatelets. On physical examination, she appeared comfortable and her body mass index was 26. The temperature was 35.3°C, the heart rate 87 beats per minute, the blood pressure 147/83 mm Hg and the respiratory rate 16 breaths per minute. There was no inguinal lymphadenopathy. On the pelvic exam, a reddish, hard, fixed, papillary, subcutaneous mass measuring 2 cm with gross bleeding was identified at the 2 o’clock position on the wall of the vaginal vestibule. It was difficult to properly examine the bleeding source externally due to the copious amount of bleeding. The bleeding could not be controlled by simple application of the pressure. The remainder of the examination was unremarkable.
Investigations
The bleeding was stabilised by arginine sodium powder. Complete blood count, liver function tests and coagulation tests were ordered, which showed the white blood cell count 8690/µL (normal 3500–12 000/µL), haemoglobin count 14.1 g/dL (normal 12.0–16.0 g/dL), platelet count 175 K /µL (normal 150-400 K/µL), aspartate aminotransferase 83 U/L (normal 8–48 U/L), alanine transaminase 90 U/L (normal 7–55 U/L), gamma-glutamyl transferase 35 U/L (normal 9–48 U/L), prothrombin time-international normalised ratio 0.96 (normal 0.9–1.1) or activated partial thromboplastin time 30.9 s (normal 25–40 s). A vaginal tumour or a cervical cancer relapse was suspected, and she was referred to a gynaecologist, who conducted a biopsy of the suspected bleeding lesion and then sprayed sodium alginate over it to stop the bleeding. The biopsy result showed squamous epithelium, interstitial cells and inflammatory cells including neutrophils but no malignant lesions. Urinary tract epithelial metaplasia was prominent in the squamous epithelium.
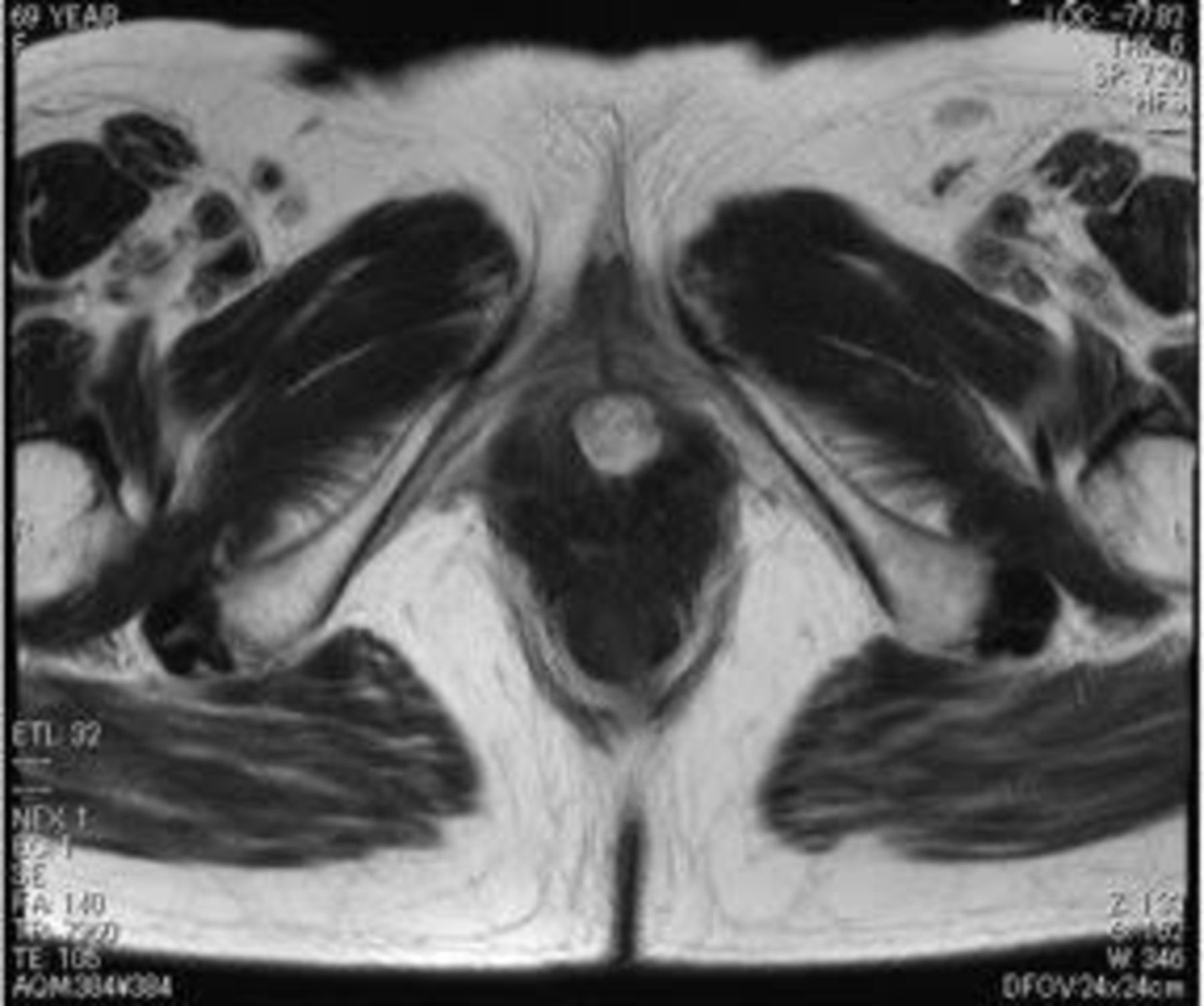
In the next visit, the gynaecologist noticed a papillary, protracted subcutaneous mass on the vaginal anterior wall and a circumferential mucosal extrophy on the external urethral orifice, exposing a urethral mass (figure 1). MRI of the pelvis with administration of gadolinium contrast in an axial T2-weighted image showed high-intensity mass (1.6 cm × 1.6 cm × 2.7 cm) arising from the posterior urethral meatus. There was no decrease in apparent diffusion coefficient, no evidence of invading the surrounding tissues or lymphadenopathy (figure 2). CT of the pelvis with administration of contrast showed a 2 cm sized mass which appeared to be located on the urethral meatus (figure 3). Both MRI and CT imaging showed no evidence of malignancy. Cystoscopy was conducted, which revealed no abnormalities in the bladder, internal ostium of urethra or urethral meatus.

Cystoscopy showed a pedunculated, reddish, 2 cm sized mass on external urethral meatus at the 6 o’clock position.

MRI of the pelvis with administration of gadolinium contrast in an axial T2-weighted image shows high-intensity mass (1.6 cm × 1.6 cm × 2.7 cm) arising from the posterior urethral meatus.

CT image of the pelvis with administration of contrast agent showing a 2 cm sized mass which appeared located on the urethral meatus.
Differential diagnosis
Differential diagnosis for lower tract bleeding in a menopausal woman after hysterectomy1:
Vaginal tumour.
Gartner duct cyst.
Condyloma acuminatum.
Varices.
Cervical cancer relapse.
Treatment
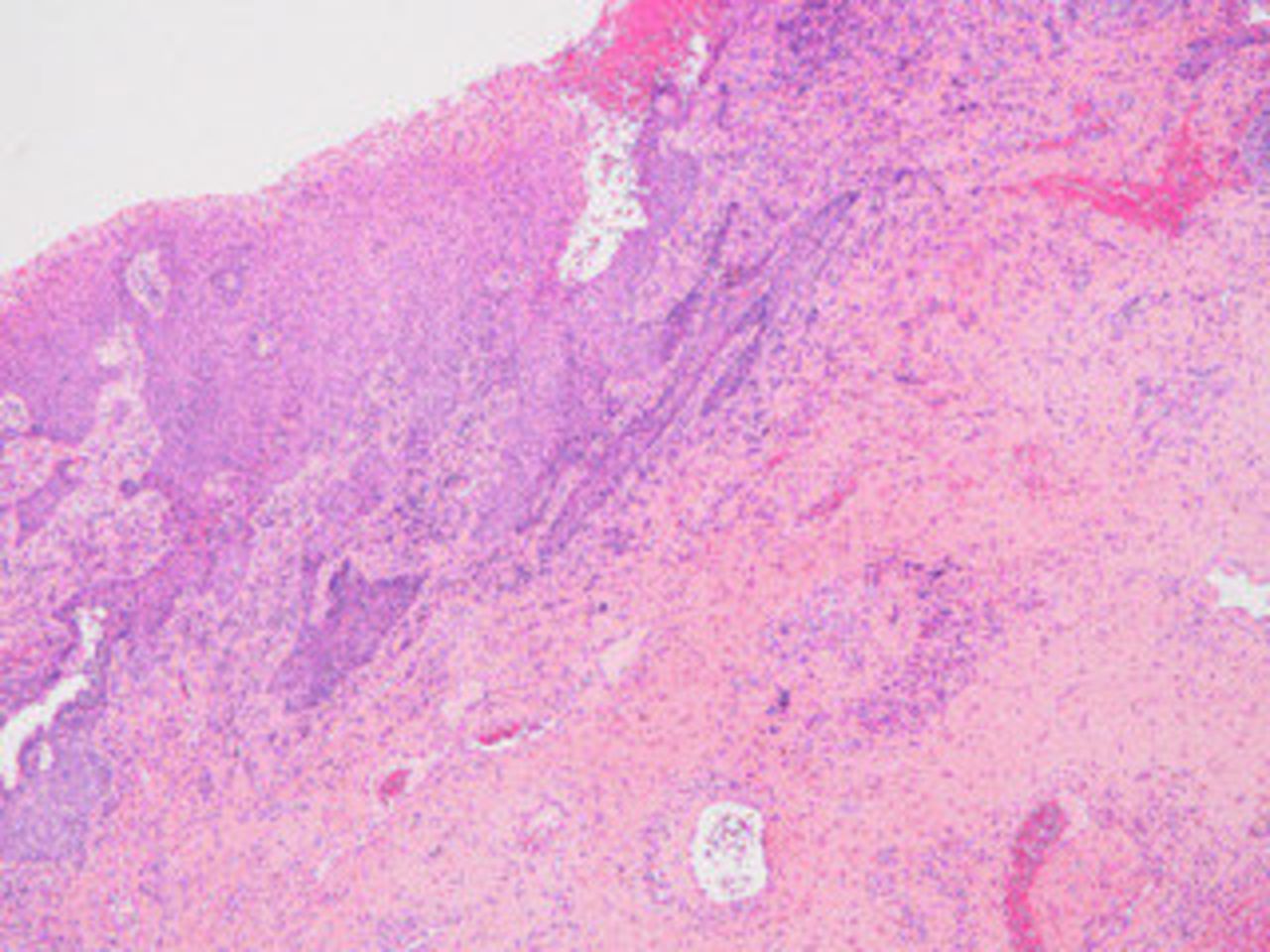
The patient was referred to a urologist and underwent surgical resection of the urethral tumour. In the surgery, the urethral tumour was resected, followed by knotted suture between mucosa and external urethral orifice wall. Urethral prolapse was repaired. A urethral catheter was placed following the surgery. On microscopic examination, there were swollen, dilated vasculatures and mild inflammatory cell invasion mixed with neutrophils, which were covered with non-atypical stratified squamous epithelium and transitional epithelium. The margin status was clear. There were no findings of malignancy (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Microscopic examination showed swollen, dilated vasculatures and mild inflammatory cell invasion mixed with neutrophils, which were covered with non-atypical stratified squamous epithelium and transitional epithelium.
Outcome and follow-up
She noticed an improvement in urination after the operative resection. By the 2-week follow-up visit, she had recovered and did not report any problems with urination as before.
Discussion
A urethral caruncle is a benign fleshy outgrowth of the posterior urethral meatus. The aetiology is still undetermined but many women with urethral caruncles are asymptomatic, and urethral caruncles are occasionally identified as incidental findings during genital examination. In a review on its clinicopathological features, the presenting symptoms were pain (37%), haematuria (27%) and dysuria (20%), in addition to them being reported as asymptomatic (32%).2
Although caruncles are recognised as benign tumours, biopsy is recommended if the mass is irregular, firm or possesses other characteristics which may indicate malignancy. Furthermore, bleeding is a common symptom among cases of urethral caruncle, but it is important to consider the possibility of concurrent and potentially malignant causes of bleeding. In a review of 394 women presenting with malignant urethral lesions mimicking caruncles, bleeding was the most common complaint.3 Malignant melanoma, urethral adenocarcinoma, non-Hodgkin’s lymphoma, tuberculosis and ovarian tumour have been reported as causes mimicking urethral caruncles.4–8 Primary malignant melanoma of the urethra is extremely rare, but early diagnosis of urethral melanoma is important due to their tendency of early metastasis.9 Careful evaluation should be performed if patients are positive for symptoms or have signs suggestive of malignancy, including the amount of bleeding, findings on pelvic exam, risk factors and response to treatment for the caruncle.
Learning points
Among cases of suspected genital tract bleeding, urinary tract lesions could be the true source of bleeding.
A urethral caruncle is a benign fleshy outgrowth of the posterior urethral meatus.
Although cases of urethral caruncle are typically asymptomatic, some may present with heavy bleeding.
Acknowledgments
Thanks to Dr Toshiya Shinohara for the pathology report.
Footnotes
Contributors KS, RK and HK cared the patient and KS and YT wrote the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.