Article Text

Statistics from Altmetric.com
- ear, nose and throat/otolaryngology
- congenital disorders
- otolaryngology / ENT
- paediatric surgery
- ophthalmology
Description
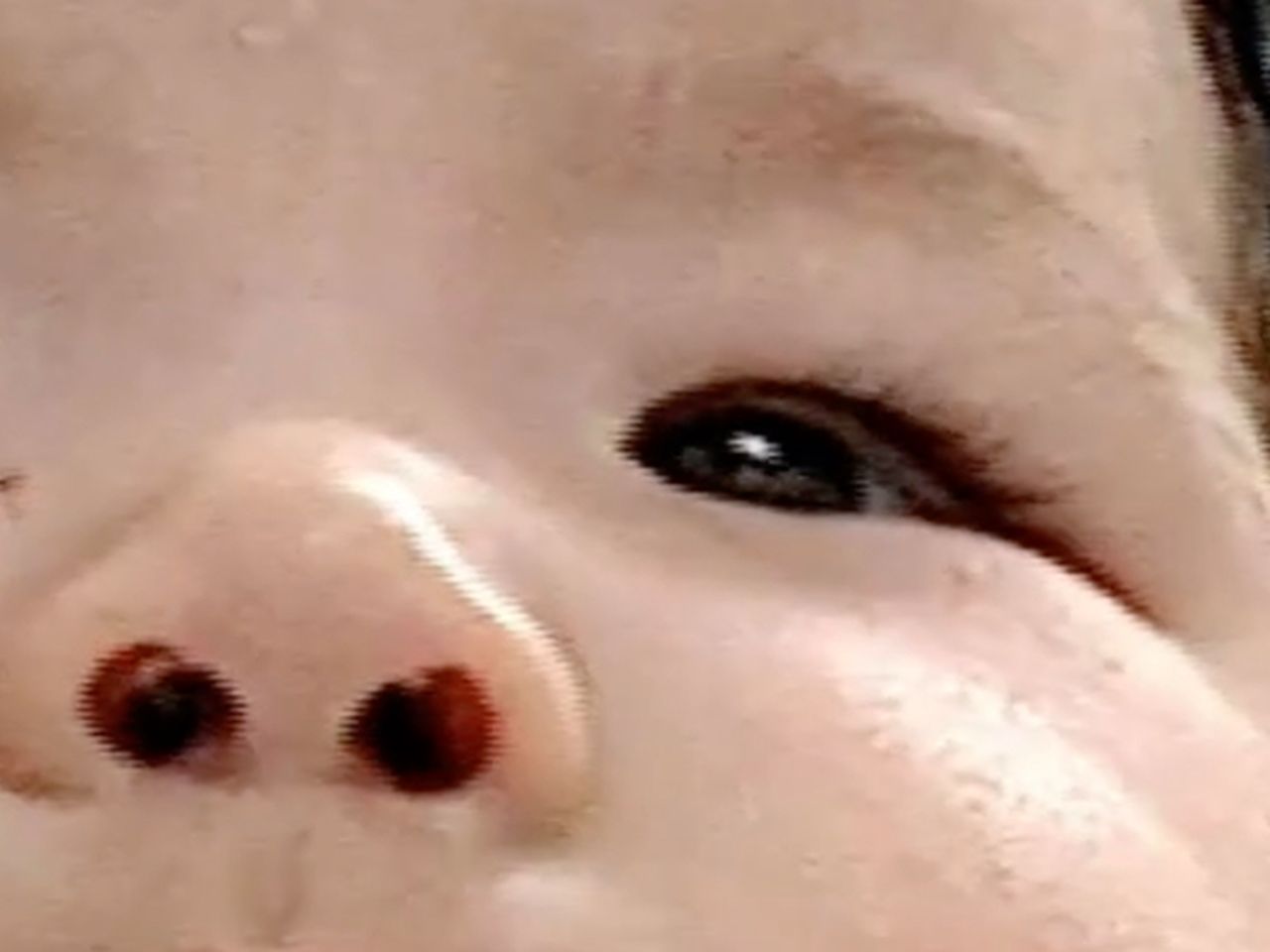
The patient was a 2-month-old girl with the primary signs of mucus discharge from the left eye and infectious swelling of the lacrimal sac. She had treated with primary concerns of mucus discharge from the left eye and infectious swelling of the tear sac. Although the eye mucus discharge improved with eye drops, the dark blue swelling in the inner corner of the left eye remained, and the patient was referred to our department. She had no difficulty breathing, there was dark blue swelling of the left tear sac (figure 1). A CT scan revealed dilation from the left tear sac to the nasolacrimal duct (figure 2).

The first examination of the patient during the initial consultation. Dark blue swelling of the left lacrimal sac was observed (yellow arrow).
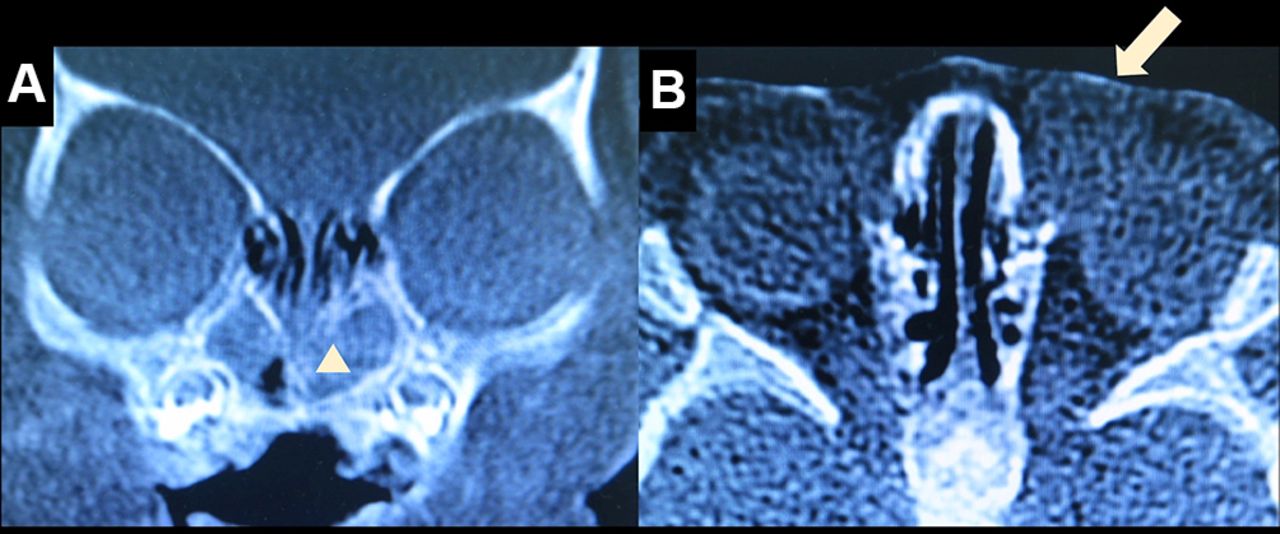
(A) The bone condition on a CT coronal section. A soft-tissue concentration shadow was observed in the left common nasal meatus (white triangle). (B) The soft-tissue condition on a CT horizontal cut. Left tear sac and nasolacrimal duct dilation were observed (white arrow).
Congenital intranasal nasolacrimal duct cysts are thought to be caused by functional closure of the Rosenmuller valve at the opening of the tear sac combined with a failure to open of the Hasner valve at the distal end of the nasolacrimal duct.1 It is a relatively rare disease, and more than 90% of cases of congenital nasolacrimal duct stenosis are expected to heal naturally.2 The basic treatment for congenital intranasal nasolacrimal duct cyst is lacrimal sac massage, but for patients with respiratory distress, vision disorders, acute inflammation and who relapse, eye drops, oral antibiotics and drip-infused antibiotics are administered. In some cases, surgical treatment is necessary.3 If the disease does not resolve naturally or develops acute inflammation, the obstruction is released through probing by an ophthalmologist or through transnasal endoscopic cyst marsupialisation by an otorhinolaryngologist.
In this case, transnasal endoscope showed the swollen section of the inferior meatus was punctured with an 18-gauge needle and drained. The section was full of pus, and we confirmed the outflow of pus and resolution of swelling of the lacrimal sac. We provided continued antibiotic eye drops and lacrimal sac massage after the intervention. The patient experienced a relapse of symptoms 1 week later, so we discussed with the ophthalmologist the risks associated with probing under general anaesthesia in the operational theatre versus those associated with endonasal marsupialisation under local anaesthesia in the outpatient department. Probing is a more common and familiar treatment compared with endonasal marsupialisation. However, using 19 Gauge ANGLED MVR Lance︎ (Feather Safety Razor, Osaka, Japan) and small through-cutting forceps, straight shaft, upwards︎ (No.10270602, Nagashima Medical Instruments, Tokyo, Japan). It is possible to make an incision safely at an appropriate site, without damaging other parts and without sedation in the outpatient department. Finally, we performed endoscopic cystic marsupialisation under local anaesthesia during an outpatient visit.
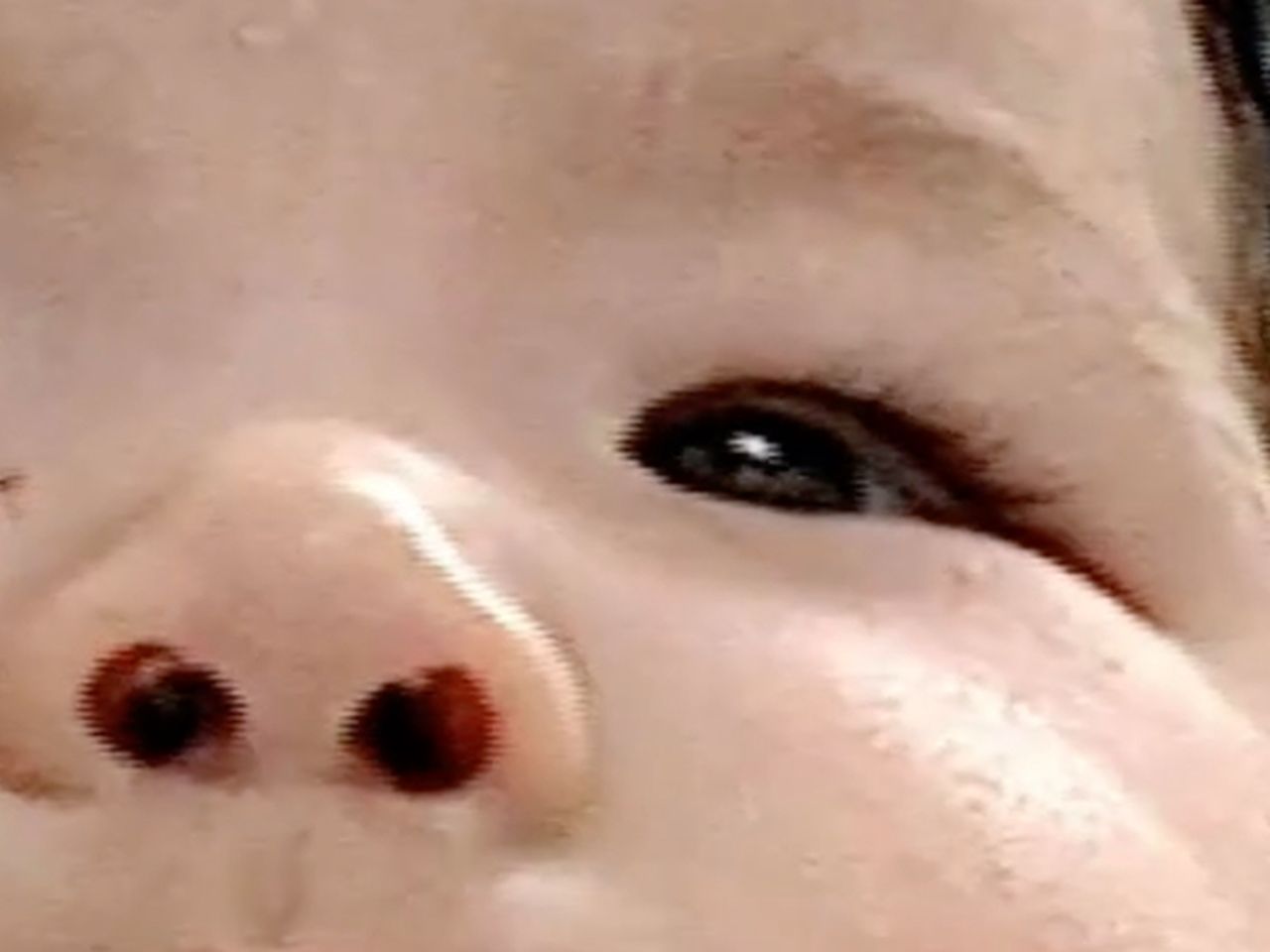
The child sits on the knee to be in close contact with the body trunk of an adult, clamps both feet of the child with both feet of an adult, holds down the arm and head with the hand of an adult. After applying local anaesthesia with xylocaine containing 1% epinephrine, the mucous membrane of the anterior end of the inferior turbinate was incised with 19 Gauge ANGLED MVR Lance︎ (video 1). The swelling from the inferior meatus was then incised, and we confirmed drainage of the inferior meatus. Sufficient marsupialisation of the opening was achieved with small through-cutting forceps, straight shaft, upwards, and the lacrimal sac was massaged to achieve complete drainage. We provided thorough aspiration during the procedure to ensure that pus did not flow into the pharynx for preventing additional stress and pneumonia. By massaging the tear sacs, we confirmed that there was no additional pus, and haemostasis and Sorbsan®︎ insertion were performed at the site of marsupialisation for continued drainage. We confirmed that there was no relapse, infection or a hernia 2 weeks after surgery (figure 3). Two years and 3 months after surgery, the patient’s nasolacrimal duct remains open.
The operational procedure of endonasal marsupialisation.
{kind=link}
{kind=link}
{kind=link}
Two weeks after surgery, dark blue swelling of the left lacrimal sac was improved.
Learning points
The basic treatment for congenital intranasal nasolacrimal duct cyst is lacrimal sac massage, but the disease does not resolve naturally or develops acute inflammation, the obstruction is released through probing or through transnasal endoscopic cyst marsupialisation.
Marsupialisation is a method that resects a part of a cyst protruding from the inferior meatus using 19 Gauge ANGLED MVR Lance and small through-cutting forceps, straight shaft, upwards in the nasal passage, where it is possible to incise the cyst in the lower nasal passage while observing the inside of the nose using an endoscope.
As probing in children above the age of 1 year requires general anaesthesia, the increased invasiveness to the child is a problem. If a cyst protruding into the nose can be confirmed, and if endoscopic cystic marsupialisation can be performed under local anaesthesia in the outpatient department, a relatively safe and less invasive surgical treatment is possible.
Footnotes
Contributors KO and NO examined the patient and diagnosed it. YS wrote the manuscript. YS, KO, NO and YT discussed the results and contributed to the final manuscript. KO supervised this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.