Article Text

Abstract
Adrenal gland infarction resulting from adrenal vein thrombosis is an infrequently recognised entity with a limited differential diagnosis. When bilateral, it can result in acute life-threatening adrenal failure. Heparin-induced thrombocytopenia (HIT) is an antibody-mediated, prothrombotic state that represents an important cause of adrenal vein thrombosis leading to associated infarction. Sometimes, the clinical picture of HIT—including the presence of HIT antibodies—occurs despite absence of proximate heparin exposure (‘spontaneous HIT syndrome’). We report a case of nearly missed adrenal failure secondary to bilateral adrenal infarction that evolved during the second week following knee arthroplasty (a known trigger of spontaneous HIT syndrome). The combination of bilateral adrenal infarction, thrombocytopenia and presence of platelet-activating HIT antibodies not explainable by preceding heparin exposure led to a diagnosis of postknee arthroplasty spontaneous HIT syndrome. The case also highlights the clinical and laboratory findings associated with rapidly progressive acute adrenal failure.
- haematology (drugs and medicines)
- adrenal disorders
- haematology (incl blood transfusion)
- immunology
- orthopaedics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- haematology (drugs and medicines)
- adrenal disorders
- haematology (incl blood transfusion)
- immunology
- orthopaedics
Background
Heparin-induced thrombocytopenia (HIT) is an adverse drug reaction with typical onset 5—10 days following an immunising heparin exposure.1 2 HIT is caused by platelet-activating IgG that recognises complexes comprised of platelet factor 4 (PF4) bound to heparin or certain other polyanions.3 HIT is highly prothrombotic (relative risk of thrombosis, 12-fold to 15-fold), with at least 50% of patients developing symptomatic thrombosis.4 5
One important complication of HIT is adrenal gland infarction, either unilateral or bilateral; when bilateral, the patient can die from acute adrenal crisis.6–8 Usually, adrenal infarction presents as adrenal haemorrhage. The unusual adrenal vascular anatomy—rich arterial inflow but only a single central adrenal vein—accounts for the special risk for adrenal infarction with adrenal vein thrombosis.8
Over the past decade, it has become recognised that patients can develop a disorder identical to HIT—including presence of ‘HIT antibodies’—despite no proximate exposure to heparin.9 10 Known as ‘spontaneous HIT syndrome’, two clinical settings are described—postinfection9–11 and postorthopaedic surgery (almost always postknee arthroplasty).12–20 We report a case of acute adrenal failure caused by bilateral adrenal infarction caused by spontaneous HIT syndrome postelective knee arthroplasty, with delayed recognition of evolving adrenal failure representing a ‘near-miss’ scenario.
Case presentation
A 68-year-old man underwent uncomplicated left total knee arthroplasty. Medical history included chronic hypertension. Antithrombotic prophylaxis with rivaroxaban 10 mg daily commenced on postoperative day (POD) 1. He was discharged home on POD 3 with instructions to continue rivaroxaban for 14 days. No heparin was administered.
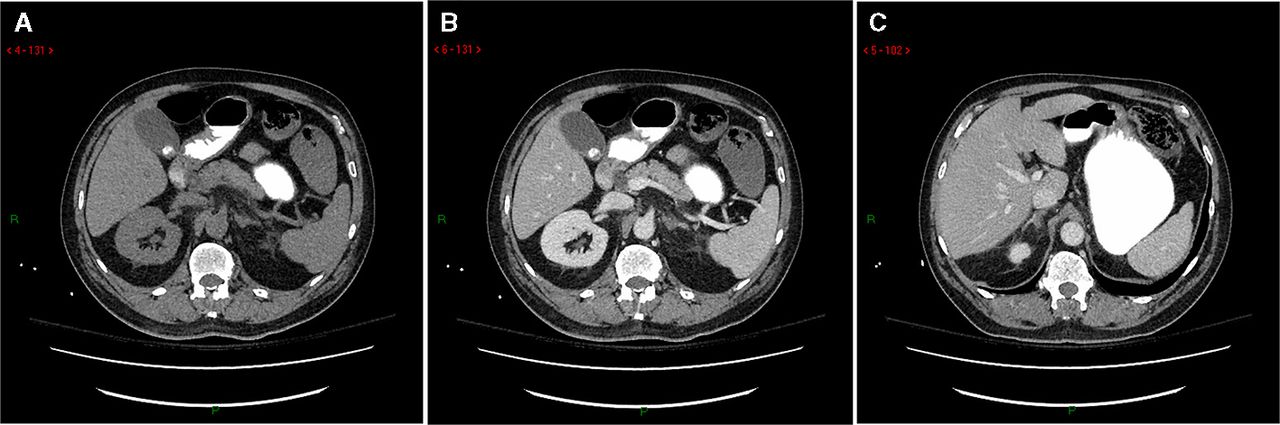
He returned to hospital on POD 8 with severe back pain radiating to both shoulders. A CT scan showed abnormal signal in both adrenal glands reported as ‘adrenalitis vs infarcts’ (figure 1). The patient was hypertensive, requiring oral (amlodipine) and intravenous (hydralazine) antihypertensive agents. Serum electrolytes were normal. Two doses of low-molecular-weight heparin (LMWH) were given for thromboprophylaxis, before switching back to rivaroxaban. His platelet count fell from 279 to 71×109/L, with the initial fall occurring prior to LMWH (figure 2). His back pain resolved, and he was discharged on POD 13, with results of an adrenocorticotropic hormone (ACTH) stimulation test and laboratory investigations for HIT still pending (see Investigations section). Given absence of clinical features of adrenal insufficiency (despite the CT abnormalities), he was not felt to require adrenal replacement therapy at discharge. However, 2 days later, he represented to hospital with new symptoms of fatigue, dizziness and vomiting; his systolic blood pressure was only 80 mm Hg despite not taking his prescribed antihypertensive medications. Adrenal insufficiency was immediately suspected, and he recovered with fluid resuscitation and intravenous glucocorticoids.

Axial CT images of the adrenals at POD 8. (A) Left adrenal precontrast and (B) postcontrast, showing adrenal swelling, inhomogeneous enhancement and oedema of periglandular fat. (C) Right adrenal postcontrast, demonstrating inhomogeneous enhancement after iodinated intravenous contrast. POD, postoperative day.

Timeline of clinical events and pertinent investigations until postoperative day 20. ACTH, adrenocorticotropic hormone; BP, blood pressure; CLIA, chemiluminescence immunoassay (Instrumentation Laboratory, Bedford, Massachusetts, USA) that detects IgG class antibodies; EIA-IgG, in-house IgG-specific enzyme-immunoassay (McMaster Platelet Immunology Laboratory) that detects anti-PF4/heparin antibodies of IgG class; EIA-IgGAM, polyspecific enzyme-immunoassay (LIFECODES PF4 Enhanced) from Immucor GTI Diagnostics (Waukesha, Wisconsin, USA) that detects anti-PF4/polyvinylsulfonate antibodies of IgG, IgA and/or IgM classes. HIT, heparin-induced thrombocytopenia; LMWH, low-molecular-weight heparin; Na, sodium; RR, reference range; U, units; UFH, unfractionated heparin.
Investigations
An ACTH stimulation test performed on POD 10 showed: baseline cortisol, 430 nmol/L, with subsequent levels of 397 and 430 at 30 min and 60 min post-ACTH, respectively, thus indicating no response to ACTH (figure 2). Despite this abnormal ACTH stimulation test, the normal baseline cortisol level was consistent with the clinical picture (hypertensive, normal electrolytes) arguing against concurrent adrenal insufficiency. In contrast, when the patient presented 5 days later (POD 15) with symptomatic hypotension and hyponatraemia, a random serum cortisol measured <28 nmol/L (normal, 80–400 nmol/L), with the corresponding ACTH level measuring 14.4 nmol/L (normal,<10.3 nmol/L), indicating symptomatic primary adrenal insufficiency.
HIT antibody results returned strongly positive (figure 2), including two screening PF4-dependent enzyme immunoassays (EIAs). Further, the platelet serotonin-release assay (SRA) yielded strong patient serum-induced serotonin release (87% and 90% at 0.1 and 0.3 U/mL heparin, respectively) with inhibition as expected at high heparin concentrations (100 U/mL). Strong heparin-independent platelet activation was shown by 83% serotonin release at 0 U/mL heparin (buffer control; see Discussion section). Screening lower-limb venous ultrasound was negative for deep-vein thrombosis.
Differential diagnosis
Although the patient’s clinical and serological picture is wholly explainable by spontaneous HIT syndrome, occurrence of bilateral adrenal infarction warrants consideration of additional contributing disorders, including sepsis (especially meningococcaemia) and other hypercoagulability states. However, blood cultures, echocardiography, CT head and MRI of the spine did not reveal infection. Follow-up testing for a chronic hypercoagulability disorder (performed 16 months postadrenal infarction), including factor VIII activity, antithrombin activity, protein C activity, free protein S, activated protein C resistance and antiphospholipid antibodies (two assays for non-specific inhibitor, EIAs for anticardiolipin and anti-β2-glycoprotein-1 antibodies), returned normal/negative.
Treatment
The patient was treated with high-dose intravenous glucocorticoids beginning on POD 15, then transitioned to chronic adrenal replacement therapy with oral prednisone (5 mg two times per day) and fludrocortisone (0.1 mg daily). He was discharged in stable condition on POD 20, and instructed to complete his prescribed course of rivaroxaban anticoagulation.
Outcome and follow-up
A follow-up abdominal CT scan 1 year later (figure 3) revealed bilateral adrenal gland atrophy consistent with previous adrenal infarction; the radiologist recommended the patient be evaluated for hypercoagulability.

{kind=link}
{kind=link}
{kind=link}
Axial CT images of the adrenals on 1-year follow-up. (A) Both adrenals precontrast and (B) postcontrast demonstrating decreased gland volume, globular shape and significantly reduced enhancement.
A haematologist (TEW) with clinical and research experience in HIT—including previous diagnoses of spontaneous HIT syndrome—reviewed the entirety of the patient’s clinical course. The timing of onset of back pain (surrogate for acute adrenal infarction) on POD 8 and falling platelet count on POD 9 that preceded LMWH administration, together with the heparin-dependent and heparin-independent serum-induced serotonin release, were considered diagnostic of postknee arthroplasty spontaneous HIT syndrome. One year after knee arthroplasty, the patient was stable on oral adrenal therapy and reported no further hospitalisations or complications. Repeat testing for HIT antibodies by SRA and EIA was negative, as expected, given the known transience of HIT antibodies.21
Discussion
Including our patient, 12 cases of postknee arthroplasty spontaneous HIT syndrome are reported.12–20 Remarkably, infarction/haemorrhage of one or both adrenal glands occurred in 8 (67%) of the 12 patients, an association that remains obscure. Our patient exhibited some noteworthy features. First, the imaging studies showed bilateral adrenal infarction without secondary haemorrhage. Second, he never developed other thrombotic manifestations of HIT (venous ultrasound was negative for deep-vein thrombosis). Third, investigations for adrenal dysfunction—including the ACTH stimulation test—were performed because of the imaging studies, and prior to symptoms/signs of adrenal failure. Interestingly, the patient clinically appeared to have normal adrenal function, and so was discharged to home without adrenal replacement therapy, representing a ‘near-miss’ scenario, as symptoms and signs of acute adrenal failure occurred 2 days postdischarge (results of the ACTH stimulation test were not available at discharge). Fortunately, he returned promptly to hospital when fatigue, dizziness and vomiting occurred, and he had obtained a home blood pressure measurement of <100 systolic (despite known chronic hypertension).
Figure 2 illustrates the timeline of evolving acute adrenal failure in this patient. Onset of bilateral adrenal infarction (POD 8) closely corresponded to the falling platelet count documented on POD 9. The ACTH stimulation test performed on POD 10 showed lack of adrenal gland responsiveness. Nevertheless, the patient did not exhibit symptoms and signs of adrenal dysfunction at that time, consistent with the normal random cortisol level obtained that day (430 nmol/L). However, he developed symptoms and signs of adrenal failure on POD 15, consistent with an approximate 7-day interval between adrenal gland infarction and onset of symptomatic adrenal failure. Perhaps release of hormones from the infarcting glands contributed to hypertension during the evolution of adrenal injury.
The pathogenesis of postknee arthroplasty spontaneous HIT syndrome is unknown. A striking feature is that only knee—rather than hip—arthroplasty—has been associated with this syndrome. This is striking because hip arthroplasty is a well-known clinical setting for developing HIT during the heparin thromboprophylaxis.22 23 Interestingly, one group of investigators24 found a higher frequency of anti-PF4/heparin antibodies in knee (vs hip) arthroplasty patients who received mechanical, rather than pharmacological, thromboprophylaxis, supporting the concept that knee arthroplasty itself can trigger anti-PF4/heparin immunisation and, rarely, development of spontaneous HIT syndrome. One feature of knee arthroplasty is that it is performed with a tourniquet; perhaps accumulation of cellular debris containing polyanionic molecules known to interact with PF4 (eg, RNA,25 DNA,25 chondroitin sulfate26) are suddenly released into the central circulation on release of the tourniquet at surgery completion, and this ‘bolus’ of polyanion initiates in some patients the HIT immune response.
Recently, spontaneous HIT syndrome has been recognised as one of several ‘autoimmune HIT’ (aHIT) disorders.27 This comprises atypical presentations of HIT (eg, delayed-onset, persisting, heparin ‘flush’-associated, spontaneous HIT syndrome) where the illness evolves independently of ongoing heparin administration (or—in the case of spontaneous HIT syndrome—any heparin whatsoever) and where the heparin-dependent HIT antibodies additionally exhibit strong heparin-independent platelet-activating properties, that is, strong serum-induced platelet activation at buffer control. Our patient exhibited these characteristic features of aHIT.
In summary, we report a near-fatal case of acute adrenal failure in a patient with bilateral adrenal infarction complicating spontaneous HIT syndrome postknee arthroplasty. The approximate 1-week interval between the onset of adrenal injury (POD 8) and occurrence of symptomatic adrenal failure (POD 15) indicates the clinical vigilance needed to prevent adverse outcomes from this unusual complication of knee arthroplasty surgery.
Patient’s perspective
I entered the hospital for what I thought was a routine knee joint replacement. The surgery went well, but my recovery was slow. I was discharged on the Friday after the Tuesday surgery, and had a fall at home; the local paramedics came in to assist me back into bed, and all seemed well. Over the next few days I slowly became quite unwell with an extreme feeling of disorientation and weakness. On the Tuesday 1 week after surgery I started to experience back pain which I put down to inactivity. On Wednesday the pain became unbearable and an ambulance was called and I was admitted back into hospital to a bed in the intensive care unit. Over the next week I had CT scans, MRI’s, and many blood tests. I also experienced projectile vomiting. Being my stubborn self I just wanted to go home thinking I would get well there. Before being discharged my blood pressure was thought high by my doctors (but lower than normal for me), and I was given some medication to lower it. I did not take this when I got home, as it did not seem what I needed. The night after returning home I started to vomit and my blood pressure continued dropping, so my wife and daughter took me back to the hospital, where I was re-admitted. I was still in the emergency ward when the lead doctor who was in charge of me in the intensive care unit came by and said they knew what was wrong with me: I had adrenal insufficiency, also called Addison’s disease. I was put on intravenous corticosteroids and admitted to a ward. I was kept in until stabilised on oral medication. I have not experienced any further major health issues since, but have had the adrenal replacement medications’ strength and type adjusted to better suit me.
My family appreciates how hard the hospital team worked to diagnose my illness and take care of me. My wife and two daughters have the same comment about feeling ignored by nurses and doctors when they wanted to express their observations of me. They have known me for a long time and feel that had they listened to their perspective of how ill I was it might have helped in some way. A family’s observations should be listened to or at least politely given some attention.
One other observation is the fact that as a patient or family member of a patient, we should be better informed of all the test results and treatments. My youngest daughter is an experienced paediatrics nurse, and it is her hospital’s policy to keep everyone fully updated, and listen to any feedback as they find it helps everyone. I was surprised to learn more than a year after my surgery, from the haematologist who reviewed my case, that my lack of adrenal function was different than Addison’s disease (an autoimmune condition), but rather explained by adrenal injury from an unusual form of HIT that rarely occurs after knee replacement.
Learning points
Back pain radiating to both shoulders (experienced by our patient) can indicate adrenal infarction.
Bilateral acute adrenal infarction should prompt consideration of a diagnosis of heparin-induced thrombocytopenia (HIT) even when perioperative heparin was not given (spontaneous HIT syndrome).
Platelet-activating HIT antibodies with the additional feature of strong serum-induced serotonin release in the absence of heparin is the serological feature of spontaneous HIT syndrome and other forms of ‘autoimmune HIT’.
There can be a delay of 1 week between onset of adrenal infarction and subsequent signs, symptoms and laboratory evidence of adrenal failure; given its life-threatening nature, clinicians should have a low threshold to diagnose adrenal failure.
References
Footnotes
Contributors EAV: patient care, consent, writing. RPT: interpretation of imaging studies, writing. APHP: interpretation of laboratory testing, writing. TEW: patient care, interpretation of laboratory test results, writing, literature review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests TEW has received lecture honoraria from Instrumentation Laboratory and royalties from Informa (Taylor & Francis); has provided consulting services to Aspen Global, Bayer, Octapharma and WL Gore; has received research funding from Instrumentation Laboratory and WL Gore; and has provided expert witness testimony relating to HIT and non-HIT thrombocytopenic and coagulopathic disorders. The other authors report no competing interests.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.