Article Text

Abstract
We present a case of a 34-year-old man with long-term diagnosis of eosinophilic oesophagitis (EoE) who did not achieve control of disease after multiple therapies including topical and systemic steroids, immune modulators and biologics. Initial endoscopic findings showed signs of active eosinophilic oesophagitis and biopsies were significant for up to 100 eosinophils per high power field during his various treatments. There was a significant improvement in the appearance of the oesophagus as well as the least number of eosinophils found in oesophagus biopsies after 3 months of treatment with tofacitinib. There are no cases of EoE treated with tofacitinib. Tofacitinib should be considered for the treatment of eosinophilic oesophagitis given its evolving role as an immunosuppressive agent.
- oesophagus
- gastroenterology
- drugs: gastrointestinal system
- endoscopy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Eosinophilic oesophagitis (EoE) has become increasingly recognised in children and adults over the last 15–20 years. Studies have shown a prevalence of EoE of 50–100 cases per 100 000 people in USA.1 Although diet, medications and oesophageal dilation continue to be current therapies for EoE. There is ongoing evaluation of the efficacy of topical steroids and biologic therapies targeting specific allergic pathways involved in the pathogenesis of EoE.2 From a treatment perspective, there is an increasing effort to minimise restriction of diet and decrease the number of endoscopies as well as to improve patient quality of life and prevention of complications.3
Tofacitinib is a Janus kinases (JAK)1/JAK3 inhibitor currently Food and drug administration (FDA) approved for treatment of rheumatoid arthritis, also used in treatment of ulcerative colitis, psoriasis, as well as renal transplantation and juvenile idiopathic arthritis.4
We report the first case of a treatment-resistant eosinophilic oesophagitis successfully managed with tofacitinib.
Case presentation
The patient is a 34-year-old Caucasian male with a history of pollen food syndrome, environmental allergies, chronic sinusitis, asthma, chronic urticarial disorder, chronic arthritis and history of oxalate kidney stones who was diagnosed with eosinophilic oesophagitis at age 25. As a child the patient presented symptoms such as projectile vomiting, allergic reactions to vaccines, failure to thrive and subsequently complained of dysphagia, epigastric pain and poor appetite. He complained of generalised rashes and hives secondary to food and environment, consequently his diet was limited to mashed potatoes, chicken and cooked carrots. His initial physical exam was remarkable for a generalised rash, inflamed turbinates. Patient had allergies to sulfa drugs, egg, fish, raw fruits and vegetables, pork and wheat. Hospitalisations occurred due to pneumonia, several bouts of sinusitis and otitis. He had several lithotripsies, nephrostomies and hip surgery, also had laparoscopic antrectomy with Billroth II due to duodenal diverticulum. He has family history of breast, stomach and colon cancer. He lived with his parents and son, never used recreational drugs or cigarettes.
Investigations
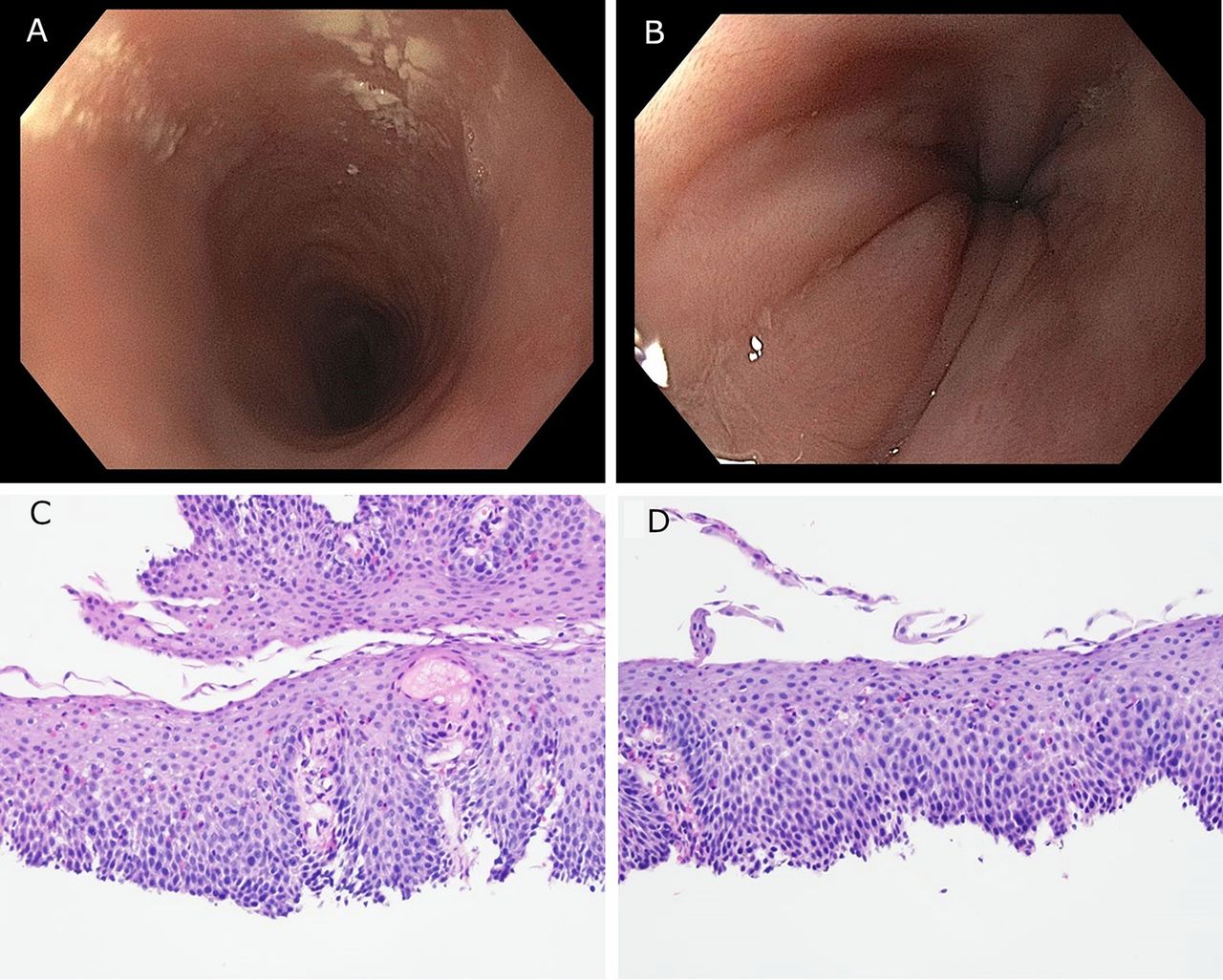
Initial endoscopy showed oesophageal mucosal changes consistent with eosinophilic oesophagitis such as ringed oesophagus, longitudinal furrows and white plaques in the proximal and mid-oesophagus (figure 1A,B). Biopsy showed squamous mucosa with marked basal cell hyperplasia, increased intraepithelial eosinophils up to 50 per high power field (HPF) and superficial distribution of the eosinophils (figure 1C and D)

(A) Oesophagogastroduodenoscopy, pretreatment proximal oesophagus. (B) Oesophagogastroduodenoscopy, pretreatment mid-oesophagus. (C) Oesophageal mucosa biopsy, pretreatment proximal oesophagus. (D) Oesophageal mucosa biopsy, pretreatment mid-oesophagus.
Laboratory investigations.
Moderate eosinophilia with 1104 cells/uL (Reference: 15–500 cells/uL) IgE level was elevated at 177 (reference: 0.0–100 IU/mL).
Interleukin Beta 174 (High) (mean 21).
Differential diagnosis
There is one condition that must be differentiated from EoE.
Gastroesophageal reflux disease (GERD): Patient did have dysphagia and endoscopic findings that often overlap with GERD except for a high number of eosinophils/HPF as well as unresponsiveness to treatment with proton pump inhibitors.
There are several gastrointestinal and systemic conditions that can cause eosinophils to infiltrate the oesophageal mucosa. These include other eosinophilic gastrointestinal disorders such as eosinophilic gastroenteritis, Crohn's disease with oesophageal involvement, pill oesophagitis, connective tissue diseases, infections (fungal, viral and parasitic), drug reactions, hypereosinophilic syndrome, achalasia, graft versus host disease and others. Our patient did not have any clinical correlation with any of these entities.
Treatment
After diagnosis was made patient was started on proton pump inhibitors (40 mg two times per day) and did not show improvement in symptoms after 6 months of treatment, patient was then started on topical steroids (swallowed fluticasone 200 µg two times per day) and he followed a restrictive diet that included mashed potatoes, chicken and cooked carrots which also did not provide any relief of symptoms. He was started on infliximab (5 mg/kg every 6 weeks) to aim for the treatment of arthritis but did not have any improvement of symptoms after three doses. He was also started on low dose methotrexate but developed an allergic reaction (severe skin rash).
Given his high level of IL-1 beta patient was started on canakinumab (150 mg every 8 weeks) due to concern for systemic inflammatory response, patient had minimal response in terms of gastrointestinal symptoms for almost 2 years as well as decreased numbers of eosinophils in oesophageal biopsies, but joint symptoms did not improve at all and decided to add an immunomodulator such as azathioprine which later induced an elevation of liver function enzymes; tacrolimus was then tried at lower doses (0.5 mg two times per day), and was discontinued after sudden onset diarrhoea after first use.
Patient was then enrolled in the RECEPTOS clinical trial (RPC4046, monoclonal antibody against IL-13) for 1 year and reported a moderate improvement of gastrointestinal and allergy symptoms, no improvement of his joint pains. The clinical trial was carried on only for 1 year and patient was in no medication for 3 months. Patient was started on tofacitinib 5 mg two times per day (with no food avoidance) and has been on this treatment until present time. Currently, patient remains free of gastrointestinal and joint symptoms.
Outcome and follow-up
Patient endorsed a significant improvement of gastrointestinal symptoms as well as joint symptoms after 3 months of treatment with tofacitinib. Upper endoscopy performed after 4 months of treatment with tofacitinib showed a normal appearance of oesophagus in upper endoscopy (figure 2A). Biopsy of the oesophagus showed much improved basal cell hyperplasia and decreased number of eosinophils to 16 eosinophils/HPF in proximal oesophagus, one eosinophils/HPF in distal oesophagus which is the lowest number of eosinophils seen in any of this patient’s endoscopies (figure 2B,C).

{kind=link}
{kind=link}
(A) Oesophagogastroduodenoscopy, post-treatment proximal oesophagus. (B) Oesophageal mucosa biopsy, post-treatment proximal oesophagus. (C) Oesophageal mucosal biopsy, post-treatment mid-oesophagus
At this time, patient remains free of gastrointestinal and joint symptoms.
Discussion
Currently, there are no published cases of eosinophilic oesophagitis treated with JAK inhibitors.
Eosinophilic oesophagitis (EoE) is a disease of chronic, allergen-driven, immune-mediated inflammation that progresses to fibrostenosis of the oesophagus if left untreated.5 Criteria for EoE includes symptoms of oesophageal dysfunction and at least 15 eosinophils per high-power field (or approximately 60 eosinophils/mm2) on oesophagus biopsy after ruling out other non-EoE disorders potentially causing oesophageal eosinophilia.6 The pathogenesis of EoE has remained unclear but some factors like genetic background, immune system and environment play an important role in mucosal inflammation and subsequent fibrosis.7
There are studies showing that EoE is associated with T helper cell-2 (Th2) type immune response to patient-specific antigens predominantly to foods. Elevated levels of the Th2 cytokines interleukins IL-4, IL-5 and IL-13, as well as mast cells, have been found in the oesophageal biopsies of EoE patients.8 Cytokines play a critical role in normal immune function and pathogenesis of immune mediated disease with the activation of JAK/STAT (signal transducer and activator of transcription) proteins pathway.
There is an evolving role JAK inhibitors as immunosuppressive treatments used in autoimmunity and transplantation medicine.4 A potential beneficial role in lessening both the epithelial inflammation and subepithelial fibrosis in EoE has been observed with JAK-STAT6 pathway inhibitors when stimulating oesophageal fibroblasts with Th2 cytokines in vitro.9
In arthritis mouse models, tofacitinib inhibits the production of inflammatory mediators and suppressing STAT1-dependent genes in joint tissue. The inhibition of both JAK1 and 3 signalling pathways was also correlated to STAT-1 suppression suggesting that tofacitinib could exert therapeutic benefit via pathways that are not exclusive to inhibition of JAK3. Polymorphisms in the regulatory regions of STAT genes have been linked with multiple immunological diseases but mechanisms are yet to be identified.4 Our patient was started on tofacitinib with the aim to control his rheumatoid arthritis and oesophageal inflammation which was achieved after 3 months of treatment. Patient had minimal gastrointestinal symptoms response to canakinumab and had moderate response to monoclonal antibody IL-13. There was significant improvement of both gastrointestinal and joint symptoms after treatment with tofacitinib when compared with both Canakinumab and monoclonal antibody IL-13. Although drugs targeting IL-5, IL- 13 and IgE are under investigation at this point, and tofacitinib has not been studied in eosinophilic oesophagitis itself, it might be helpful to investigate disease mechanisms and correlate with each patient so we can personalise therapy and improve these patients’ quality of life.
Learning points
Eosinophilic oesophagitis (EoE) is a chronic, immune mediated disease that progresses to fibrosis if left untreated. It is a global health concern in which most therapeutic recommendations are conditional and there is a need to understand disease mechanism and therapy.
Tofacitinib is a relatively new drug targeting Janus kinase (JAK)1 and JAK3 pathways interfering with JAK-STAT pathway. Tofacitinib is currently FDA approved for the use in rheumatoid arthritis and ulcerative colitis.
There is evidence that genetic mutations in JAK/STAT pathway and signalling molecules can cause immunodeficiencies and malignant cell growth.
This is the first reported case of EoE treated with tofacitinib. Our patient has been successfully treated with almost complete resolution of oesophageal eosinophilia after 3 months of therapy.
Footnotes
Contributors LBMA, XL and SG contributed to acquisition of data, analysis and interpretation of data, drafting the manuscript and critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.