Article Text

Abstract
Hirsutism is a common medical presentation to family physicians, internists and endocrinologists. Although the cause is commonly benign, a more serious or life-threatening one should not be missed. Here we report a 58-year-old woman, assessed for hirsutism and 15-pound weight gain, with associated easy bruising and mood swings. On physical examination, she was hypertensive with central obesity. Laboratory work was significant for erythrocytosis, leukocytosis with lymphopenia and transaminitis. With this initial clinical picture, a provisional diagnosis of cortisol and androgen hypersecretion was suspected. Further investigations revealed non-suppressible early morning cortisol after low-dose dexamethasone, elevated 24 hours urinary-free cortisol and late night salivary cortisol. In addition, serum adrenocorticotropin hormone was low and androgens were elevated. These results supported the provisional diagnosis and imaging of the adrenals showed a large 10.4×7.7×5.2 cm right adrenal mass, consistent with adrenocortical carcinoma, for which she underwent surgical resection.
- endocrinology
- adrenal disorders
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Hirsutism is a fairly common medical problem that affects millions of women around the world, and can cause a significant psychological burden. It is defined as an unwanted androgen-dependent hair growth in females, that is on the face, chest and back, which differentiates it from hypertrichosis, a diffuse hair growth.1 There are many causes of hirsutism, most of which are benign, and polycystic ovary syndrome (PCOS) is the cause in 3 out of 4 hirsute women.2 However, the aetiology sometimes can be life-threatening, and early detection and treatment is key to avoid detrimental consequences. Table 1 summarises the causes of hirsutism and differentiating features for each one. In this report we present a life-threatening cause of hirsutism, with elaboration on clinical features to differentiate benign causes of hirsutism from those with dire consequences.
Causes of hirsutism
Case presentation
A 58-year-old woman was assessed for hirsutism and a 15-pound weight gain over 1 year despite strict dieting and regular exercise. Her previous medical history was significant for hypertension, dyslipidemia, hypothyroidism and remote hysterectomy for fibroids. Her medications included amlodipine, perindopril, furosemide, fluvastatin and desiccated thyroid extract. The review of systems revealed complaints of tiredness, insomnia, loss of scalp hair, easy bruising and mood swings. She first noticed the weight gain and alopecia 12 months ago, but her symptoms progressed more rapidly over the last 4 months. On physical examination, the blood pressure was 152/98 mm Hg, and the body mass index (BMI) 30.8 kg/m2 with abdominal distribution of the adiposity. There was mild facial acne, sparse terminal hairs on the chin and some thinning of scalp hair. Her Ferriman-Gallwey scale for hirsutism was 11, indicating mild degree of hirsutism. On further inspection, there were isolated forearm bruises and pearl-coloured stretch marks on her abdomen.
Investigations
The initial blood work revealed an elevated haemoglobin of 172 (N: 120–152 g/L), white blood cells of 12 (N: 4–11×109/L), with lymphopenia of 0.7 (N: 1.2–3.5×109/L), an elevated alanine aminotransferase of 238 (N: 5–40 U/L) and lactate dehydrogenase of 818 (N: 110–220 U/L). The remaining liver profile, the glycated haemoglobin A1c and the serum electrolytes including potassium were normal.
Differential diagnosis
With this initial clinical picture of hirsutism, central obesity, polycythemia and lymphopenia, a provisional diagnosis of cortisol and androgen hypersecretion was suspected. Although PCOS is a much more common cause of hirsutism, late development and rapid progression along with metabolic derangements made it less likely. Further testing for Cushing syndrome (CS) revealed an early morning cortisol after 1 mg overnight dexamethasone (low-dose dexamethasone suppression test) of 707 (N:<50 nmol/L). A 24 hours urine collection for free cortisol was 3655 (N: 28–276 nmol/day) and a late night salivary cortisol was also elevated at 67.77 (N: <5.5 nmol/L). The serum adrenocorticotropin hormone (ACTH) was suppressed at 0.7 (N: 2.2–13.3 pmol/L). In addition, the serum androgens, that is, dihydroepiandrosterone–sulfate (DHEA-S), total testosterone and androstenedione were elevated at 16 (N: 0.5–5.6 umol/L), 7.7 (N: 0.1–1.4 nmol/L) and >34.9 (N: 1.0–11.5 nmol/L), respectively.
These results supported the diagnosis of an ACTH-independent cause of CS. In addition, the cosecretion of cortisol and androgen prompted the search for an adrenal tumour with a targeted MRI. A large 10.4×7.7×5.2 cm right adrenal mass abutting the medial liver edge and invading the inferior vena cava was described. These findings were suggestive of an adrenocortical carcinoma (ACC) (figure 1).
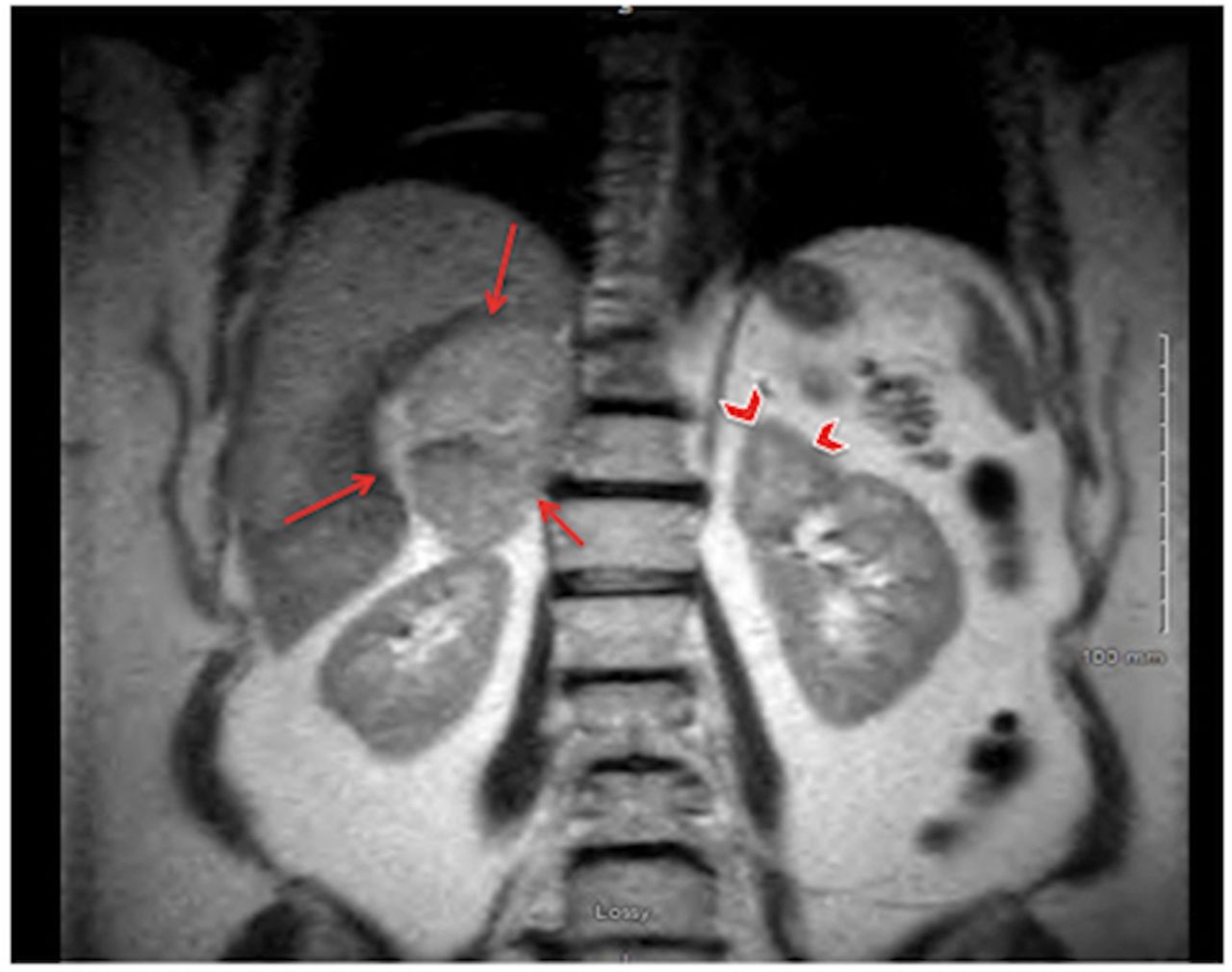
Coronal section of a T2-weighted MRI of the abdomen with contrast, showing a 10.4×7.7×5.2 cm heterogeneous polylobulated right adrenal mass (arrows) abutting the medial liver edge. In comparison, the contralateral normal adrenal gland is shown (arrowheads).
Treatment
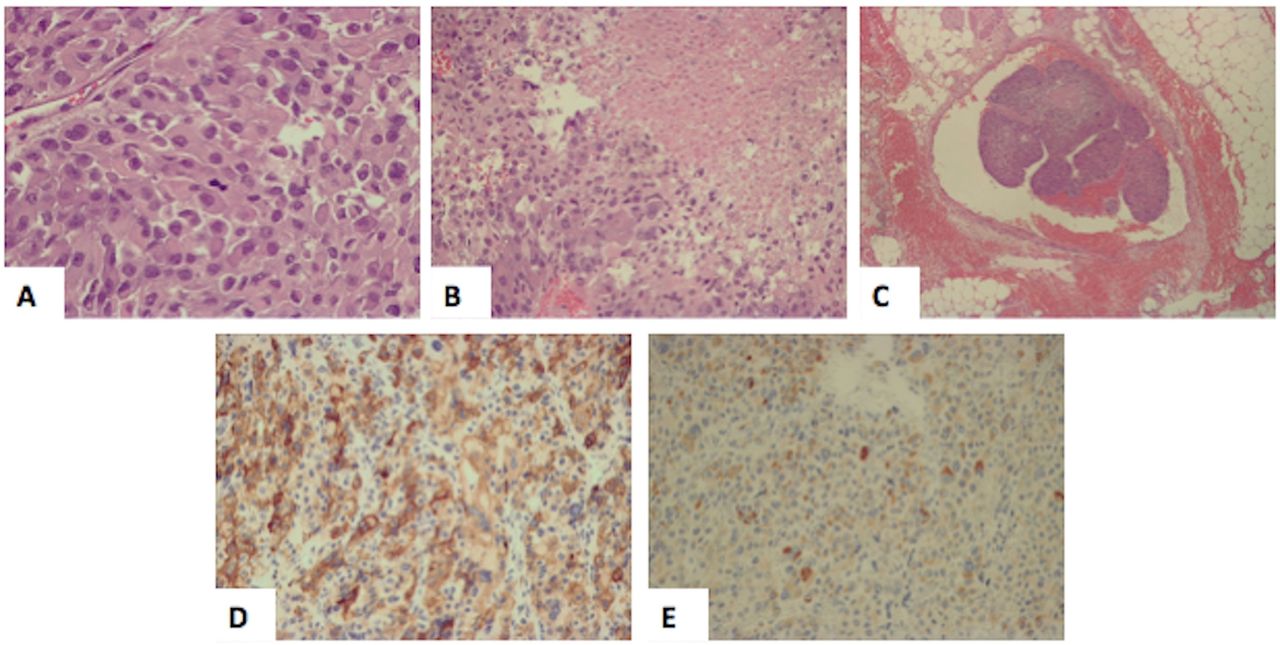
Three weeks after her diagnosis, she underwent debulking surgery with an open right adrenalectomy, inferior vena cava resection and reconstruction and cholecystectomy. The pathology results confirmed high-grade ACC of >10 cm (pT4N0) with a mitotic count of 28/50 per high-power field, Ki67 proliferative index up to 30% with vascular and liver invasion. Figure 2 shows the patient’s histopathological characteristics of her ACC along with immunohistochemistry staining confirming the diagnosis.

{kind=link}
{kind=link}
Histopathology slides of our patient’s adrenocortical carcinoma showing (A) cellular atypia characterised by nuclear pleomorphism with increased nuclear-to-cytoplasmic ratio, abundant eosinophilic cytoplasm and mitotic figure. (B) Areas of confluent necrosis and (C) vascular invasion by the tumour cells. Panels (D) and (E) are immunohistochemistry staining showing positive staining to inhibin-α and melan-A, respectively.
Outcome and follow-up
Unfortunately, with the late diagnosis and advanced disease, curative surgery was not attained and persistent residual disease was present. She was discharged home postoperatively on hydrocortisone 20 mg daily in the morning. However, given incomplete resection, early morning cortisol levels were assessed more frequently and at the 6-week follow-up visit, the cortisol level was 799 (N: 100–500 nmol/L) before the morning dose. We believed that this elevated cortisol is indicative of persistent secretion by the tumour rather than recovered left adrenal gland given it is still early for recovery of the contralateral gland and the morning cortisol level never dropped below 490 nmol/L during these 6 weeks after surgery. Based on that, her hydrocortisone was stopped, as well as her amlodipine because her blood pressure normalised.
She is currently undergoing adjuvant chemotherapy with high-dose mitotane, which is an adrenocorticolytic drug used in patients with ACC. As it will also decrease the normal adrenocortical function, glucocorticoid replacement is routinely given after initiation of mitotane. Monitoring of ACTH and urinary-free cortisol is necessary to adjust glucocorticoids dose.3 Because mitotane increases cortisol binding globulin levels, serum cortisol is not a useful marker to monitor response to therapy. One of the exceptions to routine initiation of glucocorticoids with mitotane is residual ACC, like in our patient, where monitoring for development of adrenal insufficiency is warranted before starting replacement therapy.3 Within 1 month of starting mitotane, the ACTH level has risen to 15.8 (N: 2.2–13.3 pmol/L) and the 24 hours urinary-free cortisol dropped to 40 from 236 (N: 28–276 nmol/day). She was then diagnosed with incipient adrenal insufficiency and started on hydrocortisone 10 mg orally two times per day, which was sufficient to decrease the ACTH to 1.2 pmol/L and increase the 24 hours urinary-free cortisol to 221 nmol/day.
Discussion
Hirsutism is mostly caused by excess androgen secretion either from the ovaries or adrenal glands. In premenopausal women, testosterone is produced by the ovaries, while DHEA-S is exclusively from the adrenals. Ovaries and adrenals both contribute to the production of DHEA and androstenedione. After menopause, on the other hand, the adrenals become the major source of androgens in women.4
By far the most common cause of hirsutism is PCOS, which is frequently associated with obesity and anabolic features of hyperinsulinism (hyperglycemia, hypertension and hyperlipidemia). However, when antianabolic features (thin skin, purple striae, myopathy and osteopenia) are present, this should raise suspicion for hypercortisolism (ie, CS), a less common but more serious cause of hirsutism.5
The cosecretion of androgens (DHEA-S, testosterone and androstenedione), which are anabolic steroids, mitigates the antianabolic effects of cortisol excess in the classic CS. The signs of androgen excess (hirsutism, acne, male-pattern baldness, preserved muscle bulk and bone mass and erythrocytosis) in our patient overshadowed the subtle antianabolic effects of excess cortisol (thin skin, bruising, striae and myopathy). This mixed clinical pattern prompted a search for CS with cosecretion of cortisol and androgens (a harbinger of adrenal carcinoma).
An important clue to the diagnosis of ACC was the discordant elevation of DHEA-S coupled with depression of the ACTH level. Normally ACTH drives secretion of adrenal DHEA-S and both hormones are elevated in ACTH-dependent Cushing disease and ectopic ACTH syndrome. However, DHEA-S has a prolonged half-life in serum (10–16 hours), with relatively stable levels throughout the day, making it a useful marker for the detection of chronically suppressed ACTH. Accordingly, ACTH and DHEA-S are both depressed in benign adrenal adenomas.6
ACC is a rare disorder with an incidence rate of ~1–2/million/year. There is a bimodal age distribution, that is, 1st and 5th decades of life and women are more often affected than men—59% versus 41%. On the average, the adrenal tumour measures 12 cm and weighs 689 g. Unlike adrenal incidentalomas, 80% of which are non-functional, ~60% of ACC are functional and secrete excess hormones. Cosecretion of cortisol and androgens is the most frequent pattern (~45%) and is highly suggestive of ACC.3 As with our patient, the anabolic effect of cosecreted androgens may counteract the glucocorticoids antianabolic effect on skin and muscle, thus masking the clinical diagnosis of CS.3 Unfortunately the mortality rate for advanced disease remains elevated, that is, 40% and 27.6% in stages III and IV, respectively.7
Learning points
Although hirsutism causes are mostly benign, a more serious aetiology need to be sought if progression is rapid or accompanying features and metabolic derangements are present.
The antianabolic effects of cortisol excess (thin skin, easy bruising, purple striae, proximal myopathy and osteopenia) attenuate the anabolic effects of hyperinsulinism associated with obesity and polycystic ovary syndrome and may aid in the distinction of these two disorders.
The excess production of androgens mitigates the antianabolic effects of cortisol excess in the classic Cushing syndrome.
The cosecretion of cortisol and androgens should raise suspicion of adrenocortical carcinoma.
Footnotes
Contributors SR collected data for case writing, did literature review and contributed to manuscript writing. MT contributed to manuscript writing and reviewed final manuscript before submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.