Article Text

Statistics from Altmetric.com
Description
An 84-year-old man suddenly developed dysphagia following repeated transient ischaemic attacks. He could not close his mouth, swallow food, or speak. Dislocation of the jaw, atrophy of the tongue, or gag reflex was not seen, but the snout reflex and jaw jerk were exaggerated, and the patient was able to walk. Radiological findings showed occlusion of the right internal carotid artery, leukoaraiosis and atrophy of anterior operculum. The patient's condition was diagnosed as Foix-Chavany-Marie syndrome, a type of pseudobulbar palsy.1 His mouth was kept half-open due to inability to close mouth. We used a bandage to prevent jaw dislocation and stretch the jaw closing muscles.2 Under nutritional control with gastric fistula, swallowing training was started, but dysphagia did not improve. However, vibration stimulation of the mouth with an electric toothbrush induced mastication-like movement in a reflex manner (video 1). After 2 weeks of reflex movement training, the patient was able to close his mouth voluntarily. However, adding swallowing training to the reflex movement training using an electric toothbrush failed to improve dysphagia. The mastication-like movement was analysed with surface electromyogram (EMG) by placing electrodes on the masseter, suprahyoid (digastricus) and orbicularis oris muscles (figure 1A,B). Voluntary masticatory movements were similar to the vibration-induced movements, but did not lead to swallowing movement.3 Although dysphagia of pseudobulbar palsy is difficult to treat, range of movement exercise of the mandibular joint and stimulation of the trigger point have been reported to be useful for opening the mouth and facilitating swallowing in patients with pseudobulbar palsy.4 Because of relatively abundant muscle spindles in the masseter and temporal muscles, the vibratory stimuli from an electric toothbrush probably trigger the jaw closing reflex and facilitate voluntary mastication.5 Stimulation with an electric toothbrush may be a plausible method for treating dysphagia caused by pseudobulbar palsy.

{kind=link}
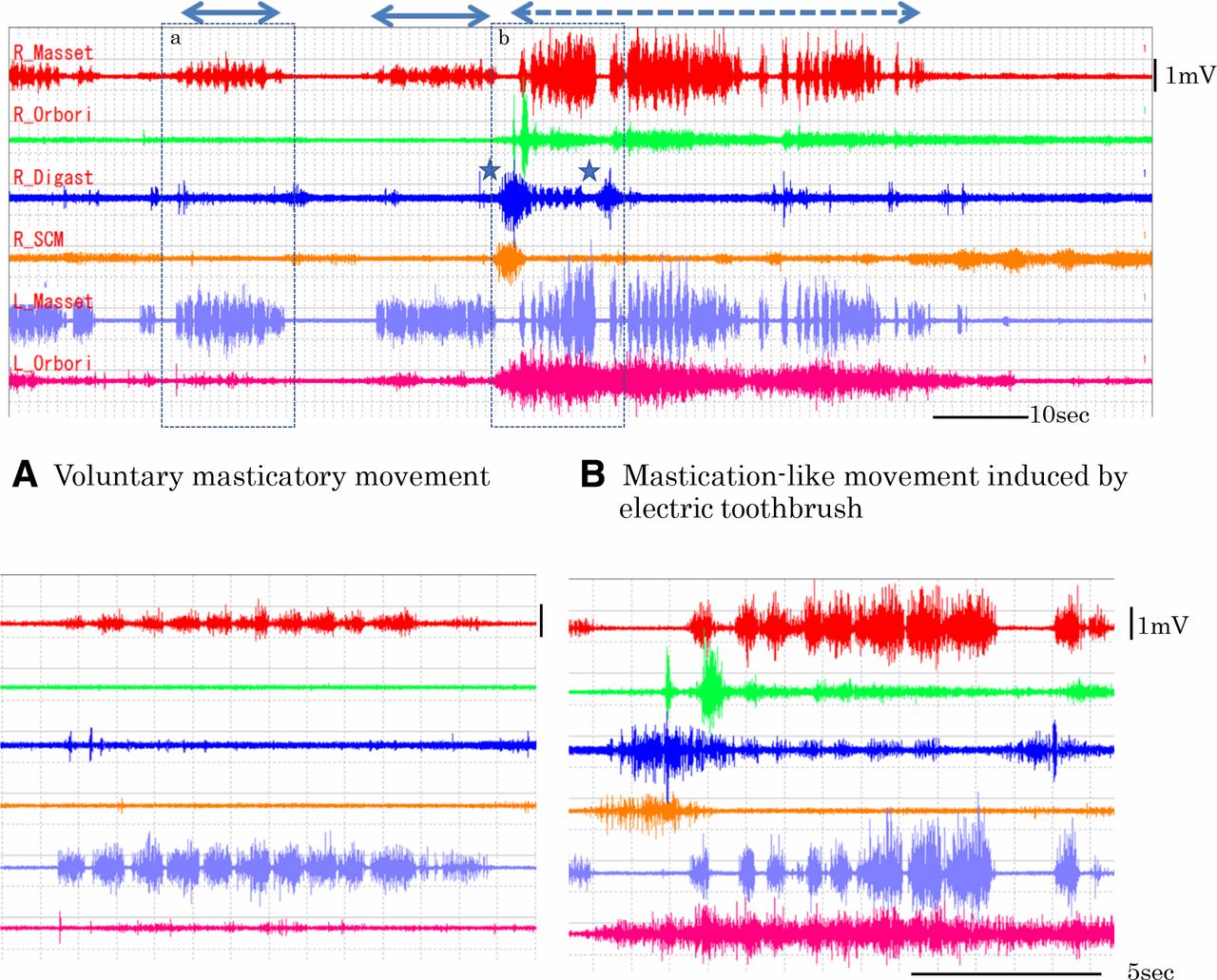
Surface EMG recorded after 2 weeks of reflex movement training when the patient became able to close mouth voluntarily and make an explosive voice. Electrodes were placed on bilateral masseter and orbicularis oris muscles, and right digastricus and sternocleidomastoid muscles. (A) During voluntary mastication, grouped discharge at approximately 1 Hz for a duration of 700–800 ms was seen in the masseters. (B) By an electric toothbrush, grouped discharges at approximately 1.2 c/s for a duration of 600–1000 ms appeared in the masseter and digastric muscles. When he held the toothbrush between his teeth, reciprocal activation and inhibition was seen between the digastricus (jaw opening muscle) and masseter (jaw closing muscle) (asterisks).
Learning points
Inability to close mouth and dysphagia caused by pseudobulbar palsy were treated by vibration using an electric toothbrush.
Mastication-like movement was induced by an electric toothbrush in a reflex manner, and voluntary mastication was possible after 2-week training.
The acquired voluntary mastication did not lead to swallowing, but vibration using toothbrush should be tried to overcome the nuisance condition of failure of closing mouth.
Acknowledgments
We appreciate Dr Yasuo Kumagai and Dr Akihiro Numao for their management of this patient in the acute hospital.
Footnotes
Contributors MN wrote the manuscript, HS made the design of this study, KK and YO assessed the effect of vibration induced mastication-like movement on the swallowing function.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.