Article Text

Statistics from Altmetric.com
Description
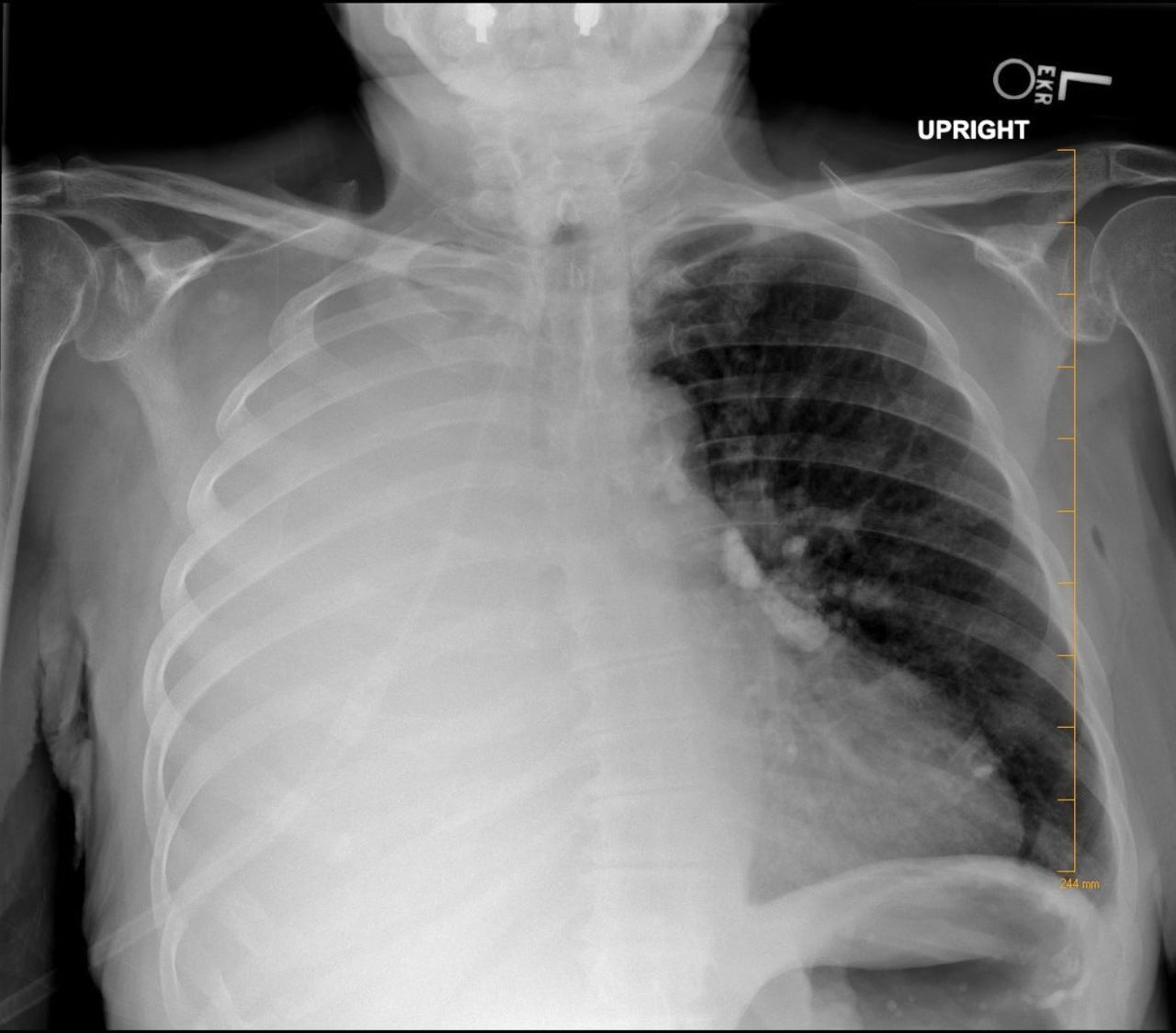
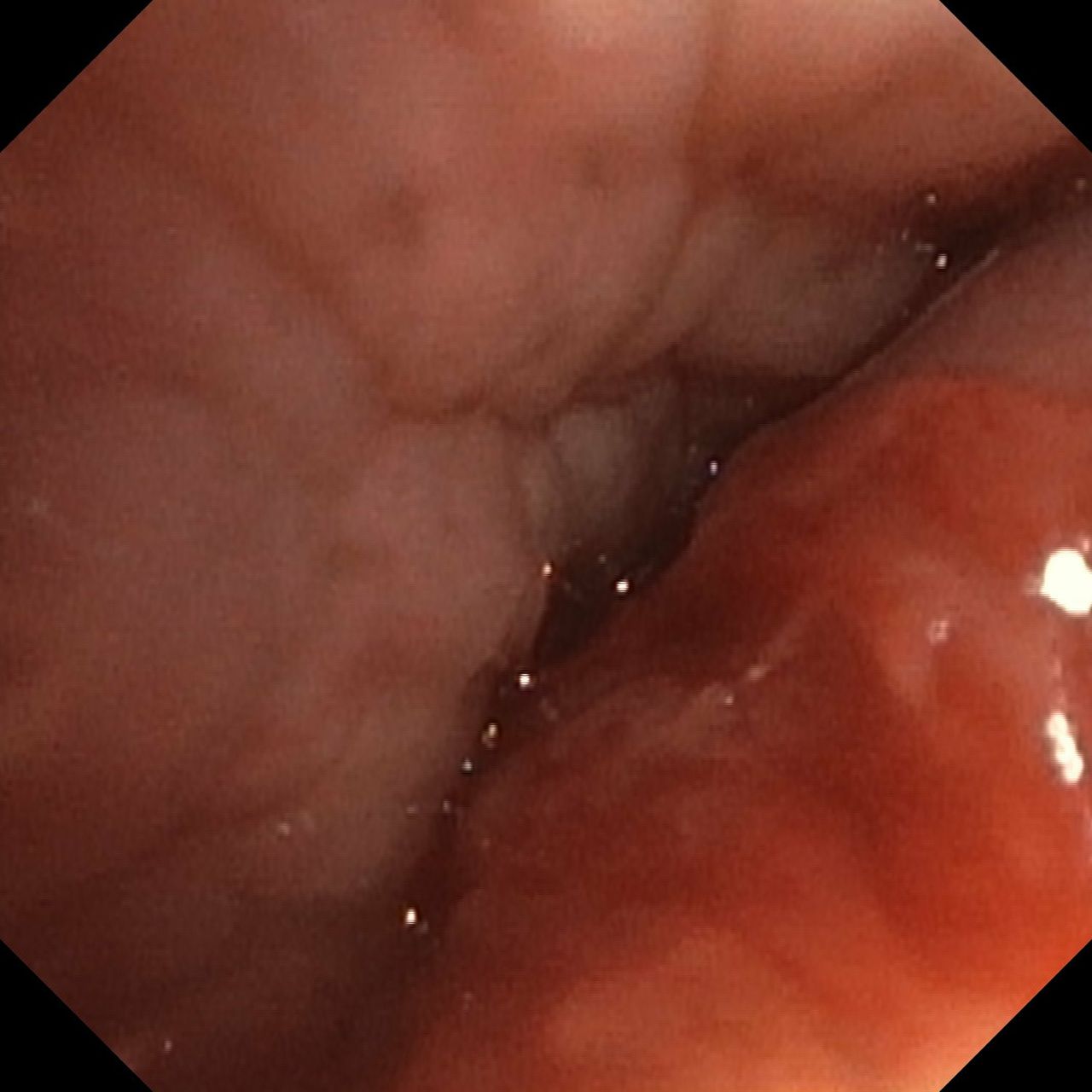
We present a 71-year-old Caucasian woman with a history of tobacco dependence who was admitted for dyspnoea and cough. The patient was hypoxic on arrival, and physical examination demonstrated diminished breath sounds over the right hemithorax. Her chest radiograph (figure 1) revealed complete opacification of the right hemithorax. A CT scan of the chest (figure 2) demonstrated a substantial right-sided pleural effusion, complete collapse of the right lung, compression of the right mainstem bronchus, but no clear evidence of endobronchial mass. She underwent thoracentesis with drainage of 1.3 L of straw-coloured pleural fluid before developing chest tightness. Fluid analysis revealed an exudative effusion and two subsequent pleural fluid cytology samples that were negative for malignancy. She underwent pigtail chest tube placement for further treatment of large right pleural effusion without successful re-expansion of the lung. Following failed re-expansion of the lung, there was increased suspicion for an endobronchial lesion. Therefore, she underwent bronchoscopy for further evaluation. Inspection demonstrated near-complete obstruction of the right mainstem bronchus from an endobronchial lesion (figure 3). Endobronchial biopsies and cytology brushings confirmed the diagnosis of moderately differentiated squamous cell carcinoma (figure 4).

Chest radiograph showing complete opacification of the right hemithorax.

(A) Coronal sections of CT scan of the chest demonstrating complete collapse of the right lung with large right pleural effusion. (B) Axial sections of CT scan of the chest demonstrating complete collapse of the right lung, compression of the right mainstem bronchus and large right pleural effusion.

Bronchoscopy image of the right mainstem bronchus demonstrating an obstructing fungating endobronchial mass.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
H&E stain of right mainstem endobronchial mass biopsy showing moderately differentiated squamous cell carcinoma.
Pulmonary atelectasis can be divided into six variants (resorptive, passive, adhesive, cicatrisation, compressive and gravity dependent); the most common type is resorptive atelectasis also known as obstructive atelectasis. This type of atelectasis occurs when there is an obstruction between the alveoli and trachea.1 2 In patients with large unilateral pleural effusions without evidence of mediastinal shift away from the effusion, physicians should begin to suspect additional aetiologies for the lung collapse in addition to compressive atelectasis. These aetiologies include freezing mediastinum due to mediastinal adenopathy and endobronchial lesions.3 Obstructive atelectasis leads to reabsorption of the air within the alveoli, leading to the opaque consolidation seen on chest radiography. A major cause of large airway obstruction is bronchogenic carcinoma.2 Squamous cell carcinoma is the second most common cause of bronchogenic carcinomas.4 In those with idiopathic atelectasis, 30%–35% are ultimately diagnosed with lung cancer.5
Large pleural effusions can lead to compressive atelectasis that results in lung collapse from extrinsic compression. Therapeutic thoracentesis should result in near complete re-expansion of the lung. In cases where there is limited lung re-expansion, the differential diagnosis includes trapped lung, lung entrapment or an endobronchial lesion.3 Exudative pleural effusions leading to compressive atelectasis require further investigation with cytological studies, as malignancy must be excluded. Unfortunately, cytological studies on pleural fluid are only positive 65% of the time, but this percentage can be increased with serial pleural fluid sampling.6 Additionally, physicians should be cautious when performing thoracentesis and should limit the amount of fluid drained when the aetiology of the effusion is unknown.7
In this case, lung collapse was initially thought to be secondary to compressive atelectasis from a large unilateral pleural effusion. However, failure to re-expand the lung with thoracentesis increased suspicion for an obstructing endobronchial lesion. Unilateral pleural effusions should warrant further evaluation with bronchoscopy to rule out an endobronchial lesion when no clear aetiology can be elicited from pleural fluid studies and re-expansion is not achieved with thoracentesis.
Learning points
Newly identified unilateral pleural effusions should warrant further evaluation by thoracentesis.
Unilateral pleural effusions should warrant further evaluation with bronchoscopy to rule out an endobronchial obstruction from malignancy or foreign body when lung re-expansion is not achieved with pleural fluid drainage.
Resorptive atelectasis is the most common type of atelectasis and results from endobrochial obstruction.
Footnotes
Twitter @ArminK0404
Contributors TPP, EMK and AK were all involved in drafting and editing manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.