Article Text

Statistics from Altmetric.com
- cardiovascular medicine
- cancer - see oncology
- ultrasonography
- radiology (diagnostics)
- lung cancer (oncology)
Description
Endomyocardial metastasis causing ST-elevation on ECG is a rare phenomenon. The most common sources of cardiac metastases are carcinomas of the lung, breast, oesophagus as well as lymphoma, leukaemia and malignant melanoma.1 Primary lung carcinoma is the most frequent source.1 2 Reports of cardiac metastasis incidence vary greatly and are described via autopsy series, ranging from 1.5% to 25%.1 2 Pericardial metastases are the most common at approximately two thirds of cases, whereas endomyocardial metastases are rare at 5%.2 Tamponade, arrhythmia, congestive heart failure and coronary artery embolism or compression with ST-elevation on ECG are known complications.1 2 We present imaging of endomyocardial metastasis from biopsy-diagnosed primary lung adenocarcinoma with biventricular mobile extensions and right ventricle (RV) apical hypokinesia presenting as ST-elevation and chest pain.
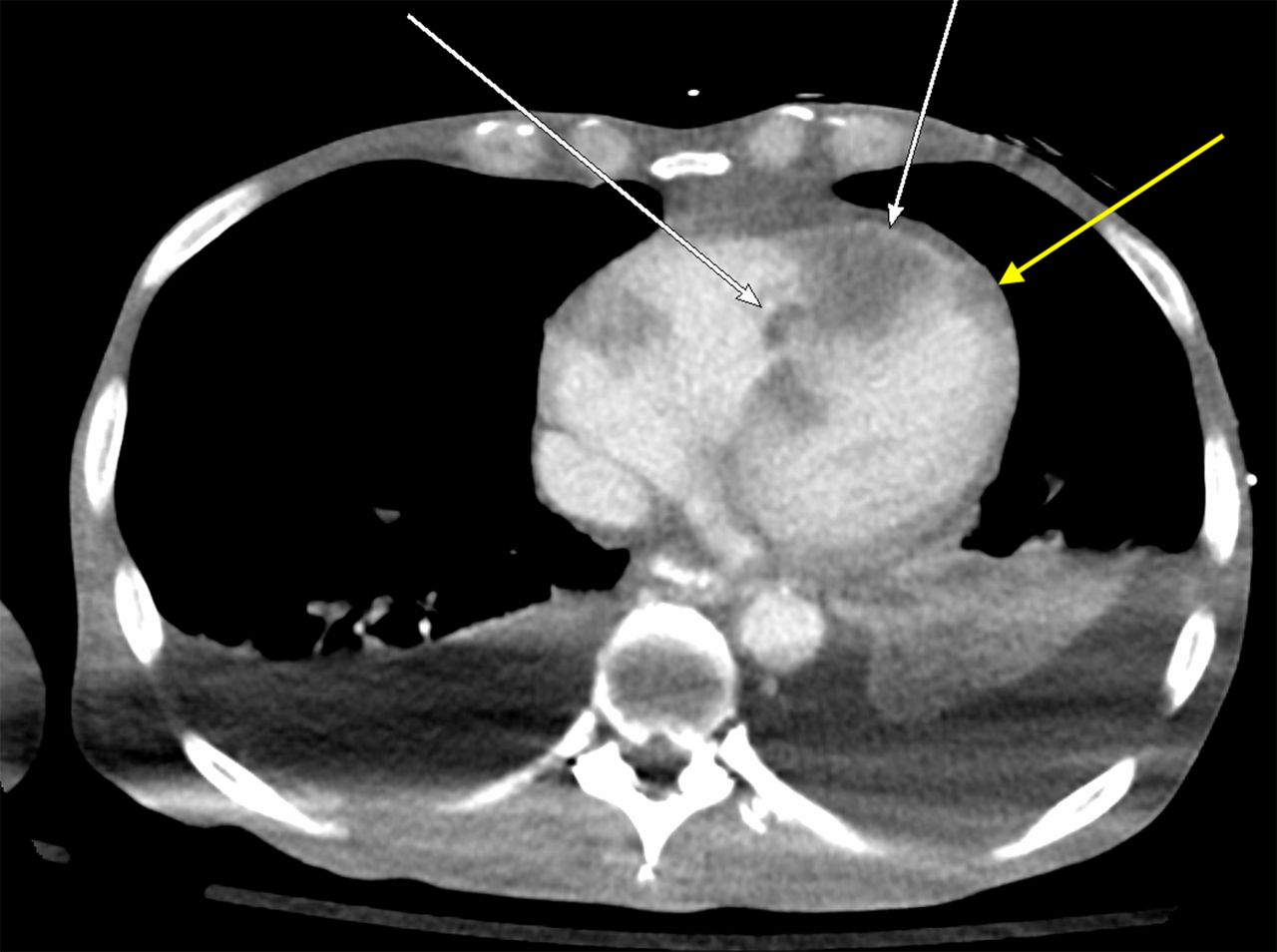
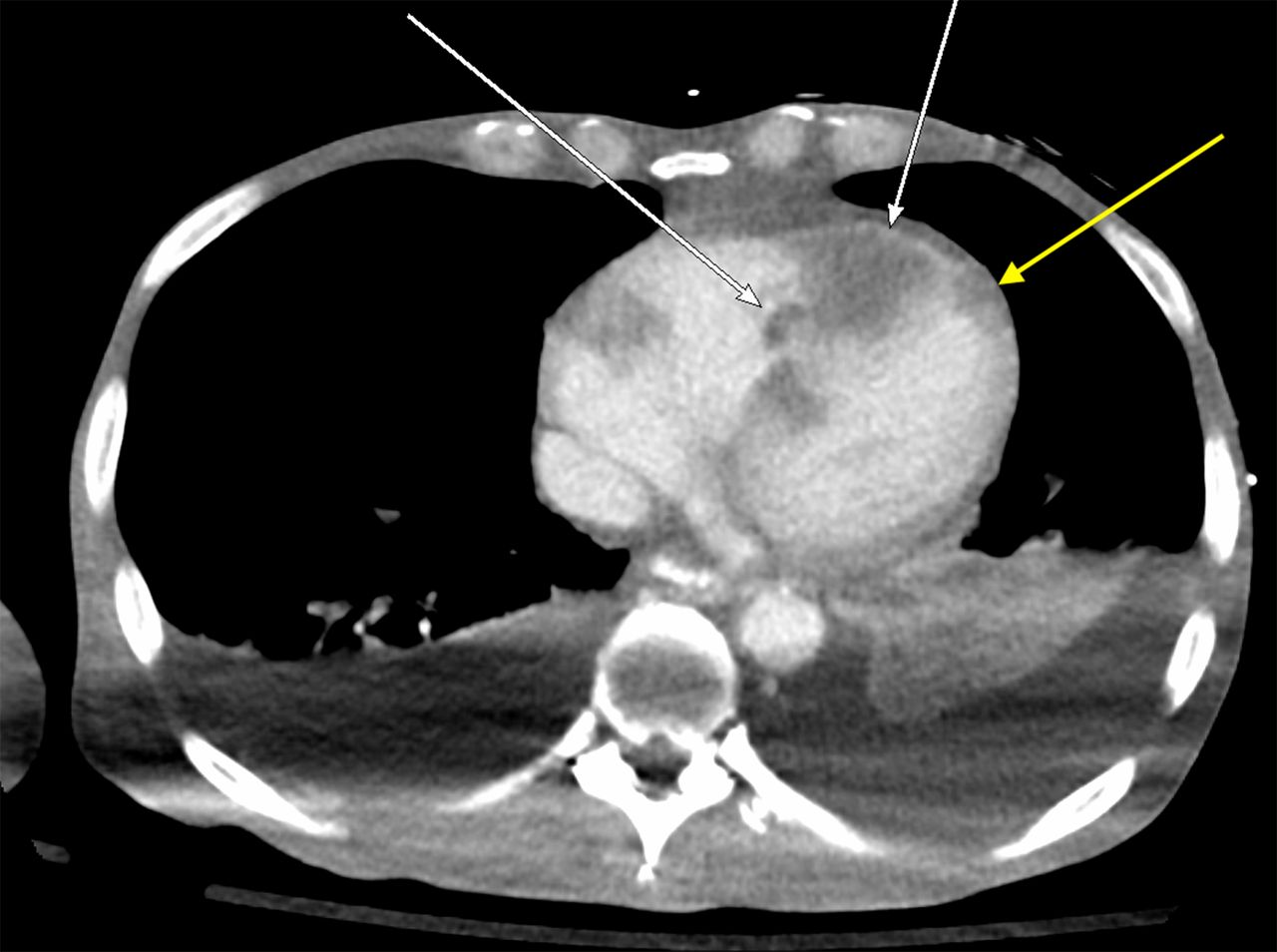
A 75-year-old man with a significant medical history of biopsy-diagnosed metastatic primary lung adenocarcinoma presented to the emergency department complaining of new-onset chest pain worsening with inspiration and shortness of breath. On presentation, his temperature was 100.2 °F, heart rate 93 bpm and blood pressure 142/125 mm Hg. Oxygen saturation was in the mid-70s, which improved with supplemental oxygen by nasal cannula. Physical examination was remarkable for bilateral axillary lymphadenopathy. ECG revealed ST-elevation in leads V3, V4 and V5 (figure 1) and labs revealed an elevated troponin of 0.06 ng/mL. Stat transthoracic echocardiogram (TTE) with definity contrast revealed globally decreased left ventricular (LV) ejection fraction calculated at 48%. A hyperattenuated mass appearing to extend from the RV apical wall into the RV cavity with mobile extensions concerning for metastatic lesions was also observed. Similar lesions were also appreciated in the LV apical wall and the pericardium. The visualised valves were normal (video 1). CT with contrast revealed hypodensities corresponding to the TTE findings with metastatic lesions in the RV myocardial wall extending into the cavity and in the LV apical wall extending into the pericardium (figure 2). Coronary angiography was not pursued as the patient’s family did not want invasive procedures. The patient was admitted to the intensive care unit where troponins trended down to normal. He was then transitioned to comfort measures per family request. Home hospice arrangements were made, and the patient was discharged in stable condition.
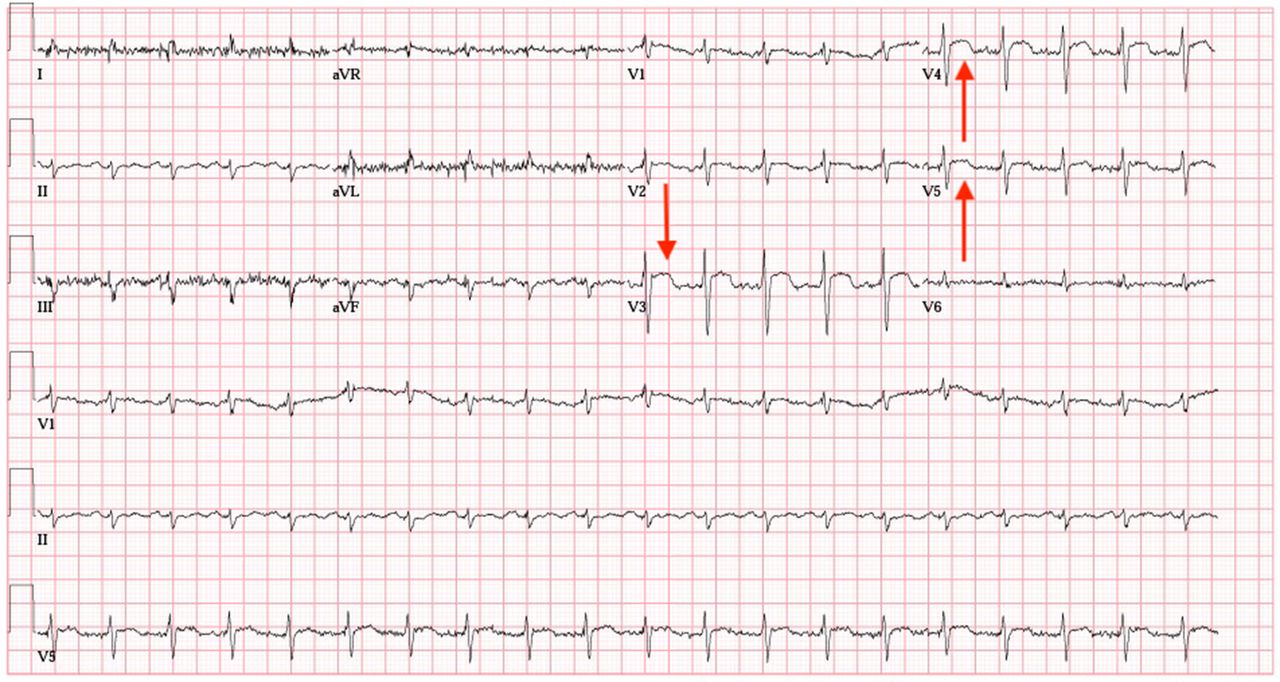
12-lead ECG revealing ST-elevation in leads V3, V4 and V5 (red arrows).
{kind=link}
{kind=link}
Contrast-enhanced CT demonstrating metastatic lesions in the RV myocardial wall extending into the RV cavity (white arrow) and in the LV apical wall extending into the pericardium (yellow arrow). LV, left ventricular; RV, right ventricular.
Definity contrast TTE demonstrating a hyperattenuating mass extending from the RV apical wall into the RV cavity with contrast-enhancing mobile extensions. Also demonstrated is a LV apical wall lesion extending into the pericardium. LV, left ventricular; RV, right ventricular; TTE, transthoracic echocardiogram.
Endomyocardial metastases large enough to produce new-onset ST-elevation on ECG often correlate to transmural metastasis and are rare.1 2 In such cases, persistent ST-elevation in precordial leads without evolution (Q wave development) has been suggested to be characteristic.1 2 TTE is most often the modality by which cardiac metastases are discovered. Echo contrast agents provide excellent information regarding the composition of visualised cardiac masses. Malignant, highly vascular masses have been shown to enhance with contrast when compared with thrombi which do not enhance.3
Naturally, as this case corresponds to metastatic disease, cardiac metastasis mimicking ST-elevation myocardial infarction indicates a poor prognosis.1–3 We therefore describe the rare phenomenon of the biventricular metastasis of primary lung adenocarcinoma presenting as ST-elevation.
Learning points
Cardiac metastases most frequently arise from primary lung carcinomas. The pericardium is most commonly the site of metastasis, but rarely the myo- and endocardium may be involved.
Most cardiac metastases from primary lung carcinomas are small and asymptomatic. Lesions large enough to produce ECG changes and symptoms suggestive of ST-elevation myocardial infarction are rare and correlate to transmural metastasis.
Echocardiography is the modality of choice for the discovery and study of metastatic cardiac lesions. Echo contrast agents demonstrate enhancement of malignant and vascular masses. Findings are often supported by contrast-enhanced CT or cardiac MRI.
Footnotes
Contributors YA was the cardiology fellow taking care of the patient. J-YRN was the medical student in the CCU contributing to the care of the patient. BAK was the internal medicine resident in the CCU taking care of the patient. MD was the attending cardiologist overseeing and directing the care of the patient. All authors involved contributed equally to the production of this submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.