Article Text

Abstract
A 68-year-old man on apixaban presented to the emergency department with back pain following a long-haul flight. Investigations for pulmonary embolus and aortic dissection were negative and he was discharged with analgesia for mechanical back pain. He presented three more times with worsening back pain, third time with urinary retention and the fourth time with lower limb weakness and loss of coordination. He was found to have a spinal subdural haematoma on MRI and transferred to a tertiary centre, where he was managed conservatively and discharged for rehabilitation with good neurological recovery.
- neurology
- spinal cord
- neurological injury
- back pain
- neurosurgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
This is an unusual case presentation of a rare form of iatrogenic back pain that was initially missed in the emergency department (ED). The patient presented multiple times with similar symptoms that progressively worsened and developed neurological deficits. Any patient that presents numerous times within a short time frame should be seen as a red flag, especially if they are anticoagulated.
Case presentation
A 68-year-old man normally fully independent with a history of atrial fibrillation, controlled with apixaban, presented to the ED with sudden onset mid-back pain following a long-haul flight. There was no history of trauma. He was investigated for suspected pulmonary embolus (PE) given the history of recent air travel, however D-Dimer was not raised and observations were stable. His pain self-resolved with no focal neurology present. He was discharged with analgesia and a diagnosis of mechanical back pain.
He represented 2 days later with a more severe recurrence of the pain through his shoulder blades, described as a ‘burning’ pain. Due to new nature of the pain, new onset hypoxia seen on arterial blood gas and stiff calves, a CT aortogram was performed to rule out an aortic dissection or PE. As there was no evidence of dissection on the imaging, he was discharged with antibiotics for a presumed infection as some reactive lymph nodes were found.
He presented for the third time the next day as a primary care referral due to urinary retention. 1300 mL of urine was seen on bladder scan and he was successfully catheterised. At this time normal power and sensation in his lower limbs were noted and there was normal anal tone on rectal examination. After an assessment by urology it was thought the retention was secondary to constipation, having started codeine recently. Bowels had last opened 3 days previously and an enema was administered in the ED with satisfactory results. He was discharged with laxatives and an indwelling catheter.
The following day after his third discharge he presented for the fourth and final time, with headache, neck stiffness, vomiting and dramatically reduced coordination in his lower limbs. On examination he was alert with no photophobia or confusion, and normal power and sensation in his upper limbs. However, power and coordination were reduced bilaterally in his lower limbs and reflexes were difficult to elicit. A broad-based, ataxic gait was observed. He was admitted and apixaban was stopped due to a clinical suspicion of haemorrhagic spinal pathology. Urgent CT of his head showed a small possible subarachnoid haemorrhage and MRI of his spine was initially reported by the radiologist as showing a thoracic syringomyelia in T1–T5 (figure 1), with extension in L4–S1. However, this was later determined to be a spinal subdural haematoma.
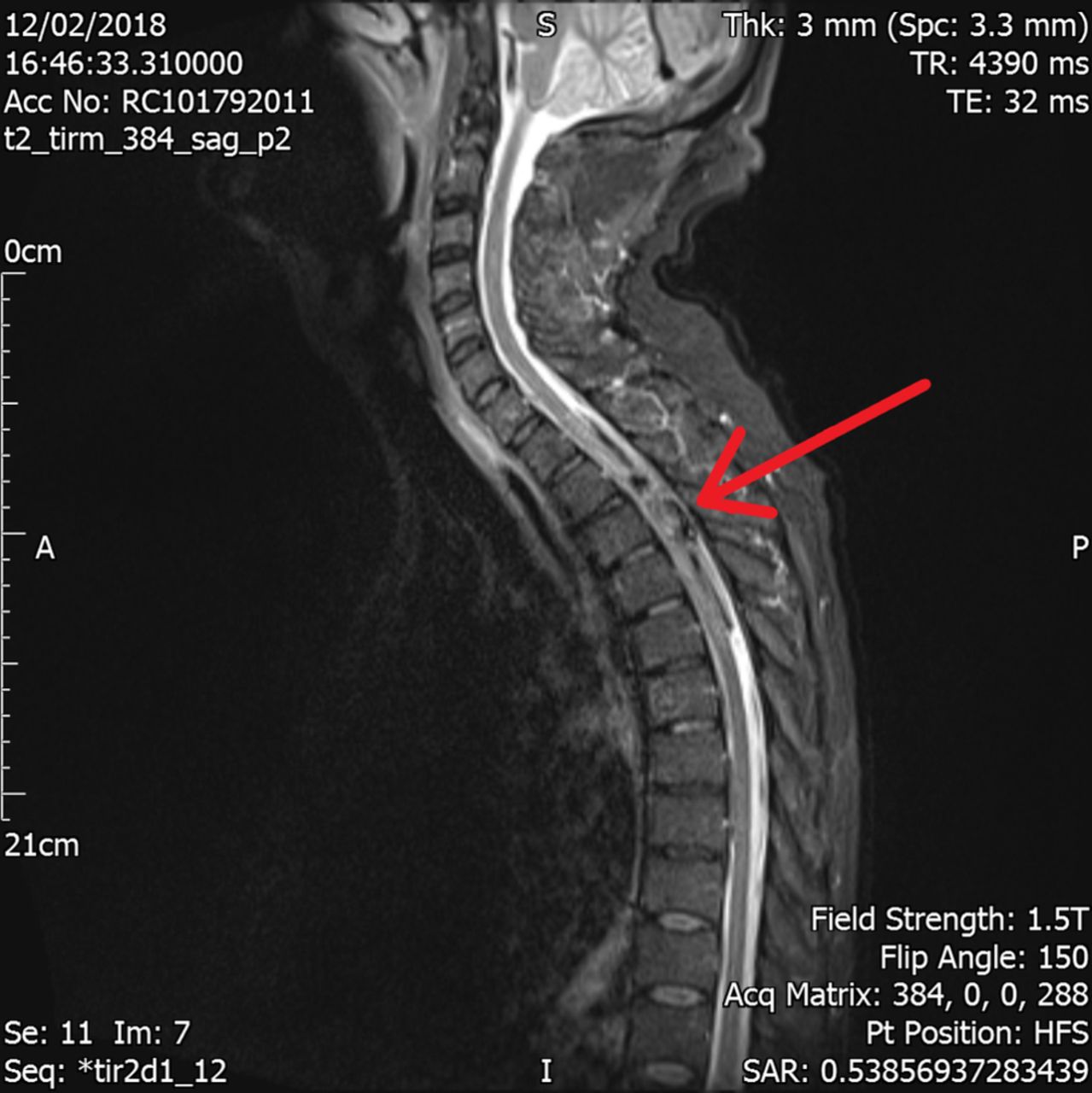
T2-Weighted MRI of cervical and thoracic spine showing a subdural haematoma (highlighted by arrow) from T1 through to T5.
After being transferred to a tertiary neurosurgical centre, he was discussed in the spinal multidisciplinary team meeting. The decision made was for conservative management due to the bleeding risk of operating, and that this was a subacute presentation by the time he was transferred; reversal of symptoms were thought to be unlikely with surgical intervention. Had this been an acute presentation it was more likely that reversal of apixaban and surgical intervention would have been carried out. Further imaging was requested to determine if there was a vascular abnormality. Spinal angiogram was abandoned due to intraoperative complications. CT angiogram and magnetic resonance angiogram were performed instead, which showed no vascular abnormality. He remained neurologically stable and was discharged to a spinal injury rehabilitation centre. He made a good neurological recovery and is doing intermittent self-catheterisation with no bowel disturbances. Mobilisation is aided with a tripod stick indoors and a wheelchair outdoors. Repeat MRI 1 month following the initial imaging demonstrated near complete resolution of the haematoma (figure 2).

{kind=link}
{kind=link}
T2-weighted MRI of cervical and thoracic spine demonstrating almost complete resolution of the haematoma (highlighted by arrow) in the T2–T3 regions.
Investigations
Bloods.
CT aortogram.
CT head.
MRI.
CT angiogram.
MR angiogram.
Differential diagnosis
PE.
Aortic dissection.
Cauda equina.
Arteriovenous malformation (AVM).
Outcome and follow-up
Referred to spinal injury rehabilitation centre. Good, but not complete, neurological recovery with conservative management. Patient performing intermittent self-catheterisation and mobilising with assistance. Repeat MRI showed near complete resolution of the haematoma.
Discussion
Spontaneous spinal subdural haematoma (SSDH) is an extremely rare cause of back pain and often irreversible spinal cord injury. The first known non-traumatic case was described in 1948 in a 16-month-old boy1; thought to be secondary to familial haemophilia. While there have been reported cases of SSDH associated with novel oral anticoagulants (NOACs) such as rivaroxaban,2–5 there has only been one other reported case associated with apixaban6 thus far to the best of our knowledge. In a recent literature review7 of SSDH looking at 122 case reports, 48% of patients had underlying coagulopathies (either through medication or acquired). However, no patients in this series were reported to be on NOACs; the majority of the medication-induced coagulopathy was due to coumarins.
A similar case to ours published in 2017 described a case of spontaneous, non-traumatic SSDH in a patient taking rivaroxaban.8 The patient developed flaccid paraplegia in her legs a few hours after taking rivaroxaban and the decision was made to perform urgent surgical decompression, after consulting with their haematology department regarding haemostasis concerns. Theoretical guidance was given to control bleeding and the patient underwent spinal decompression with preoperative prothrombin complex concentrate (PCC) and tranexamic acid (TXA) to aid haemostasis. The operation was deemed successful in removing the haematoma and perioperative haemostasis was acceptable, however the patient failed to make a neurological recovery.
Urgent surgical intervention of acute SSDH may be complicated by patient use of anticoagulants, as demonstrated above. Emergency reversal of warfarin9 and heparins10 have been well documented, however there were no definitive reversal agents of NOACs until andexanet alfa was trialled in 2015.11 A comprehensive review12 published this year explored the reversal of all classes of anticoagulants and highlighted the encouraging results seen by andexanet alfa in trials such as ANNEXA-4.13 A current ongoing trial, ANNEXA-4 is evaluating the efficacy of andexanet alfa in patients on NOACs with acute major bleeding. A perioperative assessment tool of coagulation status in patients on apixaban was developed by Thrombosis Canada14 and based assessment on biochemical markers such as anti-factor Xa calibrated to apixaban; a robust marker of anticoagulation while on apixaban.15 Preliminary analysis of ANNEXA-4 has found that anti-factor Xa activity was reduced by 93% in patients on apixaban. Owing to the promising results, the Food and Drug Administration approved andexanet alfa for reversal of bleeding in patients who are anticoagulated on rivaroxaban and apixaban in May 2018.16 There are scant studies regarding reversal of NOACs for urgent surgery either through the protocol using PCC and TXA, suggested by the authors of the prior case report,8 nor by andexanet alfa. Despite this, evidence-based clinical resource hubs such as UpToDate suggest using andexanet alfa as a first line reversal agent for all NOACs.17
As reported by the aforementioned literature review,7 presentation to the ED has been found to be most commonly motor deficits and pain. The most common location for the SSDH is the thoracic spine. There is still no agreed consensus on the best method of management for SSDH, however a comprehensive systematic review found that 86% of cases had a favourable outcome with conservative management, compared with 47% of cases where patients underwent surgical management.18 It is recommended from this review that conservative management may be preferable for patients with mild neurological deficits. As more data becomes available regarding the use of andexanet alfa in the context of surgical intervention, there may be more scope for immediate surgical intervention in the case of future acute SSDH presentations. However, we feel our case also demonstrates that in certain cases, conservative management may also lead to a positive outcome.
Learning points
Iatrogenic haemorrhage should be considered in any patient that is anticoagulated and has presented with pain.
Early diagnosis and referral to neurosurgical unit greatly increases the chances of good neurological recovery.
Conservative management may be sufficient in certain cases.
Consider with holding anticoagulation until any form of haemorrhage has been ruled out.
Early surgical intervention in patients on novel oral anticoagulants may now be possible with the use of andexanet alfa, however more data will be needed on the safety of this in the case of emergency reversal.
Acknowledgments
Since the initial submission, affiliations have changed due to job rotations within a training programme. Dr Ahmad Mchaourab is currently a ST5 Specialist Registrar in Emergency Medicine at Luton and Dunstable University Hospital. Dr Gwenllian Ying-Huey Rees Evans is a FY2 in Vascular Surgery at Bedford General Hospital.
Footnotes
Patient consent for publication Obtained.
Contributors AM contributed to the conception of the work, obtaining patient’s consent to request confidential data, contacting the tertiary centres for the acquisition of data, analysing and interpreting data and obtaining the patient’s consent to submit the final version of the report for publication. GYHRE contributed to drafting the report, reviewing and extracting the included images. All three authors contributed to critical revision of the report. RA contributed to general advice.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.