Article Text

Statistics from Altmetric.com
Description
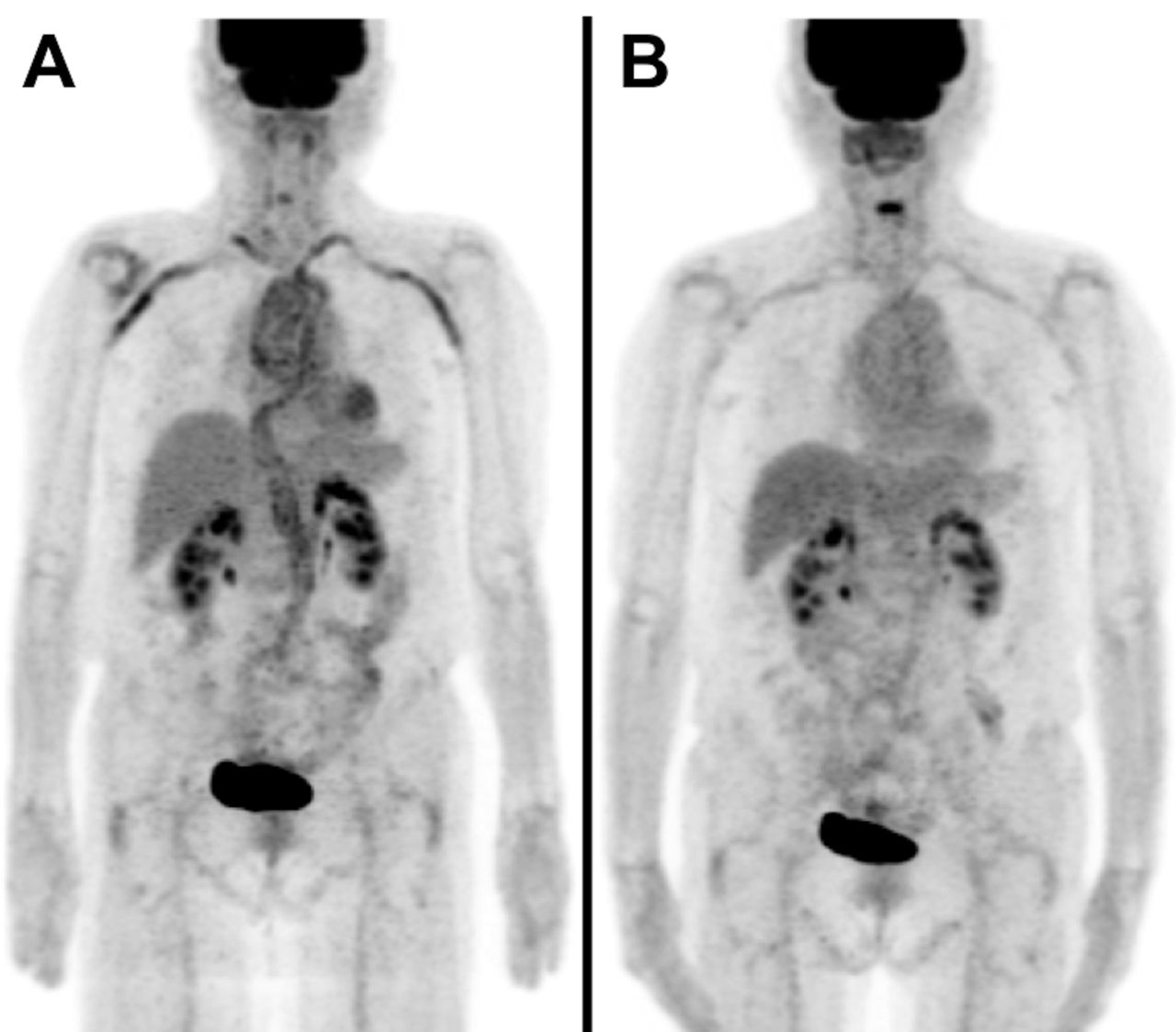
A 77-year-old Japanese woman presented with bilateral temporal headache. She had a 9-year history of rheumatoid arthritis (RA) treated with methotrexate (8 mg weekly), and a 10-year history of type 2 diabetes mellitus treated with sitagliptin and glimepiride. She had mild cognitive impairment (normal Mini-Mental State Examination score) but no fatigue, weight loss, jaw claudication or vision loss. Physical examination of the chest and abdomen was unremarkable. No swollen or tender joints were evident, and she was evaluated as having low RA clinical disease activity. She had a body temperature of 36.8°C, blood pressure 155/88 mm Hg and pulse 82 beats/min. Laboratory investigations revealed C-reactive protein 61.4 mg/L, haemoglobin 89 g/L, leucocyte count 4.65×109/L (neutrophil count 2.46×109/L), and platelet count 213×109/L. Liver and renal function tests were normal. Haemoglobin A1c was 7.0%. Serum complement C3 and C4 concentrations were normal. Antinuclear antibody and antineutrophil cytoplasmic antibody tests were negative. Urinalysis showed no haematuria or proteinuria. Ultrasound examination of the temporal artery showed the ‘dark halo sign’, indicating hypoechoic swelling around the temporal arteries bilaterally. Enhanced CT revealed diffuse wall thickening in the thoracic aorta. Positron emission tomography (PET)/CT revealed high accumulation of 18F-fluoro-2-deoxyglucose (FDG) in both subclavian arteries and in the thoracic and abdominal aorta (figure 1A). Giant cell arteritis (GCA) was diagnosed based on these characteristic symptoms and imaging abnormalities. The patient was started on subcutaneous injections of tocilizumab 162 mg once weekly at outpatient visits. Glucocorticoids were withheld because of her diabetes and the difficulty of introducing insulin therapy because of her cognitive impairment. Methotrexate was discontinued after three injections of tocilizumab because of neutropenia and to avoid further risk of complications. The subcutaneous injections of tocilizumab were continued by healthcare professionals once weekly at outpatient visits. The temporal headache gradually improved on tocilizumab monotherapy. There was no uptake of FDG in the arteries on PET-CT, indicating complete resolution of GCA (figure 1B).

{kind=link}
Positron emission tomography/CT images before (A) and 6 months after (B) initial treatment with tocilizumab. Complete resolution of the increased tracer uptake seen in both subclavian arteries and in the thoracic and abdominal aorta before treatment is evident after treatment.
Tocilizumab combined with glucocorticoids inhibits relapse of GCA during glucocorticoid tapering.1 Tocilizumab helps to decrease the cumulative glucocorticoid dose and may promote glucocorticoid-free remission in patients with GCA. Our patient responded well to tocilizumab monotherapy, with improvement seen on FDG-PET-CT. There have been other reports of GCA being successfully treated with tocilizumab alone, although evidence is limited.2 3 Tocilizumab monotherapy may improve vascular inflammation in some patients with GCA. More reports are needed to establish the appropriate regimen for tocilizumab in this disease.
Patient’s perspective
I appreciate that you identified my disease and treated it properly. I hope your report goes well.
Learning points
Tocilizumab combined with glucocorticoids is reported to inhibit relapses of giant cell arteritis (GCA) during glucocorticoid tapering.
Tocilizumab monotherapy may improve vascular inflammation in some patients with GCA.
Footnotes
Contributors TA and YM involved in conception or design of the work. TA is responsible for acquisition of data. TA, SF, TM and YM are responsible for analysis and interpretation of data. TA and YM drafted the manuscript or revised it.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests All authors received scholarship donations from Chugai.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.